Downloaded 127 times
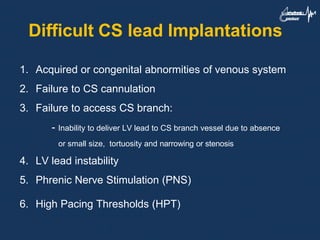
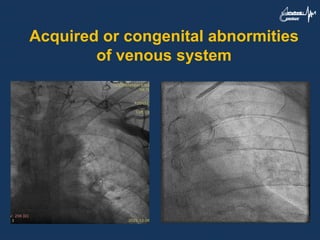
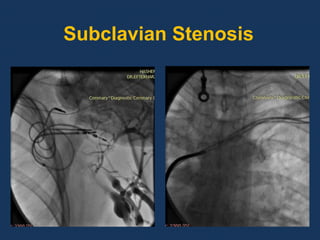
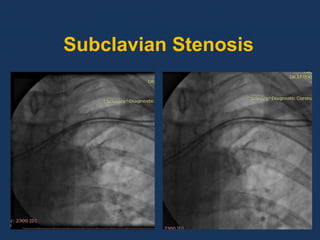
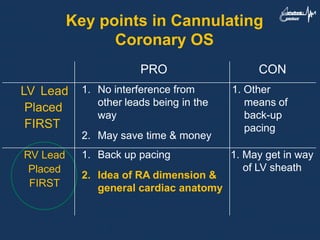
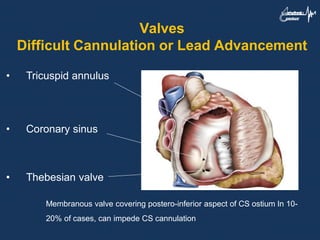
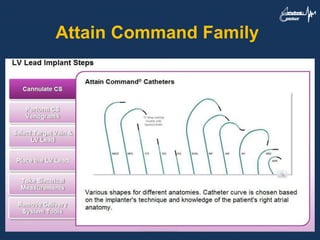
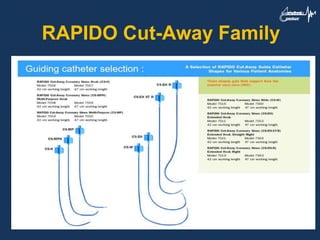
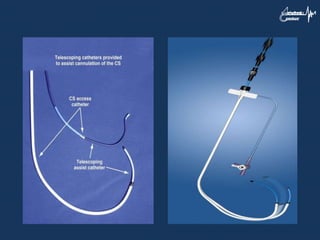
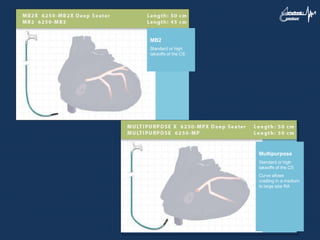
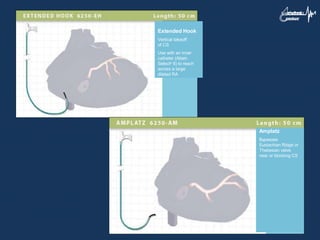
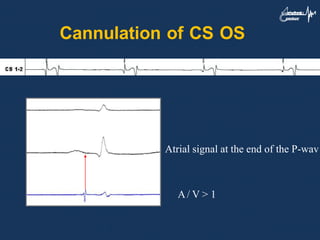
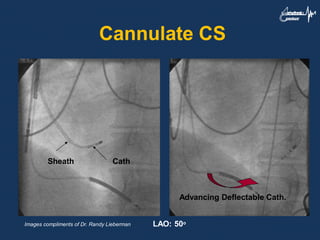
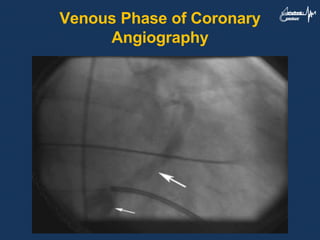
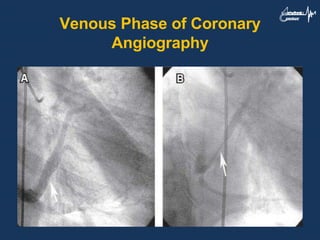

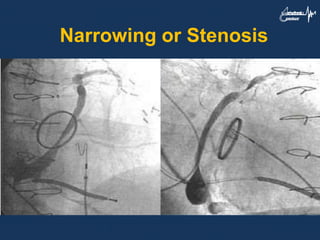
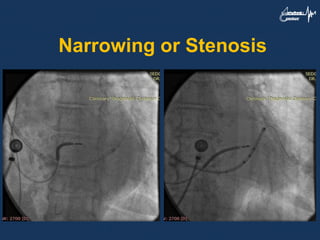
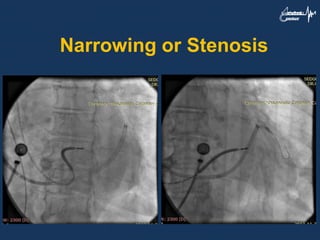
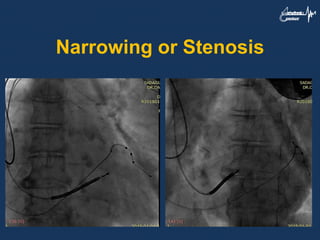
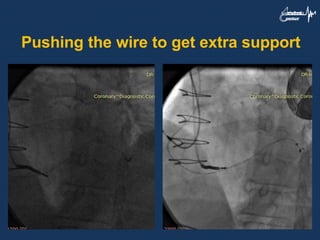
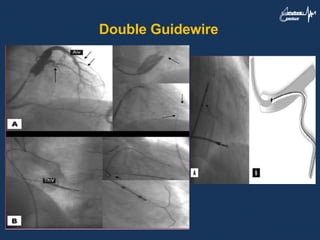
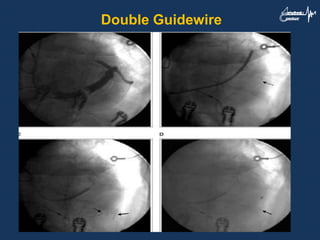
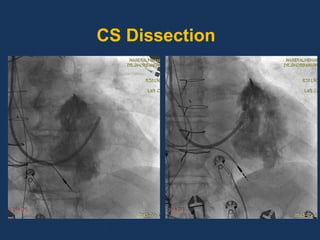
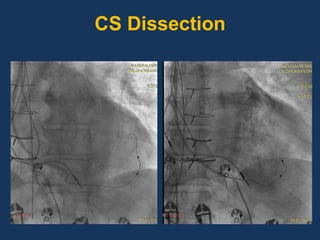
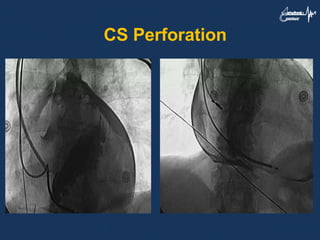
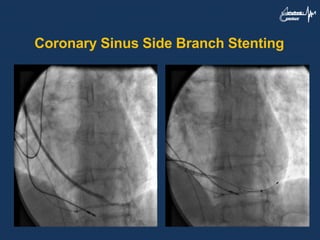
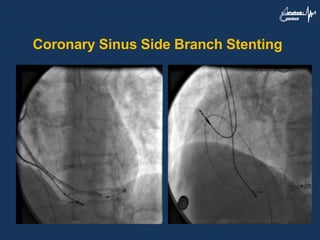
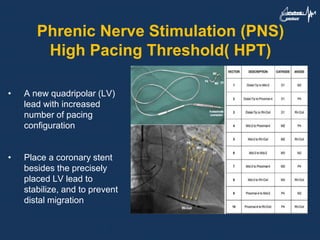
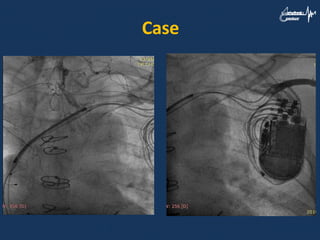
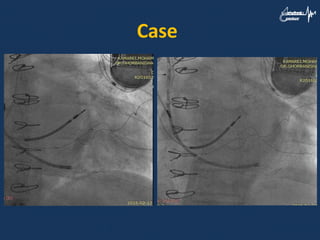
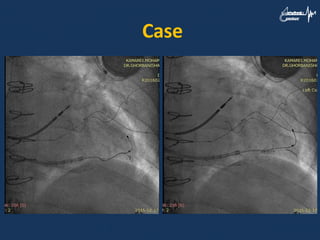
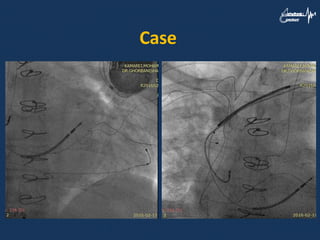
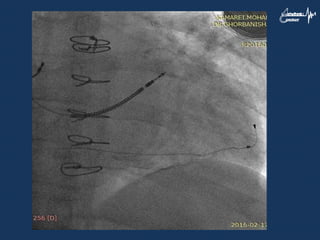


The document discusses challenges that can occur during coronary sinus lead implantation for cardiac resynchronization therapy, including anatomical abnormalities, difficulties accessing the coronary sinus or its branches, lead instability, and complications like phrenic nerve stimulation or high pacing thresholds. Specific challenges covered include stenosis, tortuosity, small vessel size, failure to cannulate, dissections, and potential solutions using devices, angiography, and stenting. The document also presents a case example of a patient who experienced left ventricular lead dislocation after initial successful cardiac resynchronization therapy device implantation.



































































