Download to read offline

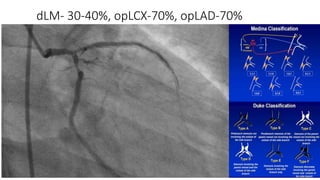
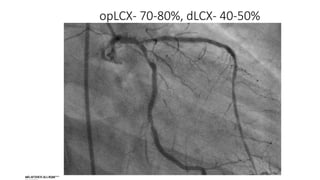
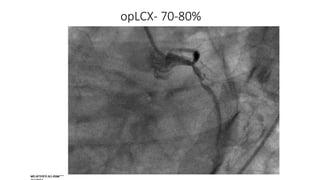
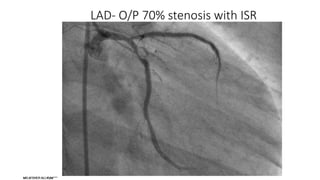


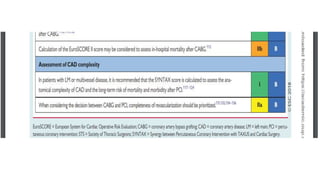
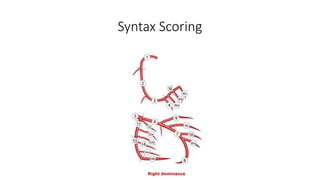
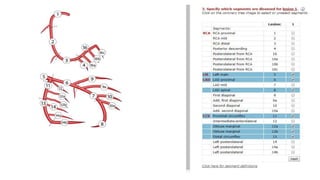


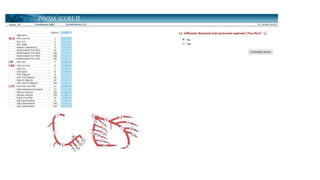
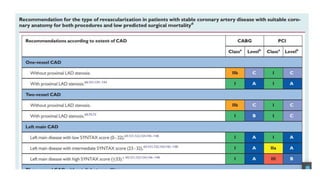
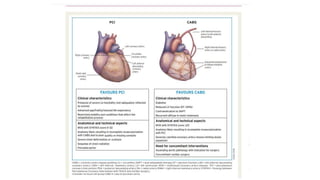
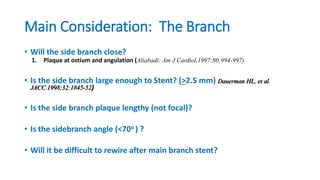
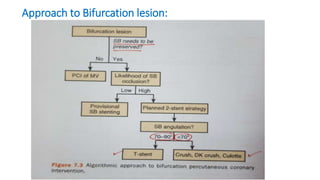

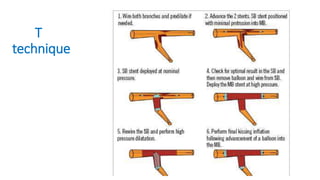
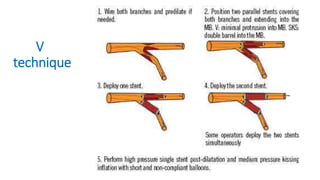
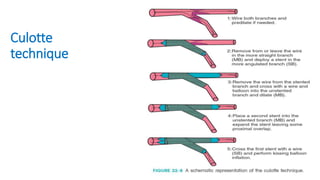
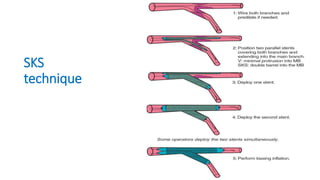

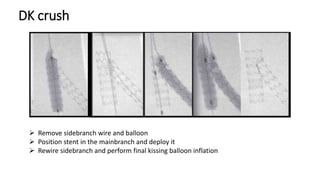

This document discusses strategies for percutaneous coronary intervention (PCI) of coronary artery bifurcation lesions. It outlines considerations for revascularization versus medical optimization and discusses stenting techniques including provisional stenting, T/V/Culotte techniques, crush techniques (classic, mini, double kissing crush), and the importance of final kissing balloon inflation. Guidelines, wiring sequence, predilation, and intravascular ultrasound guidance are also reviewed. Successful results and unsatisfactory results are defined.



































































