


































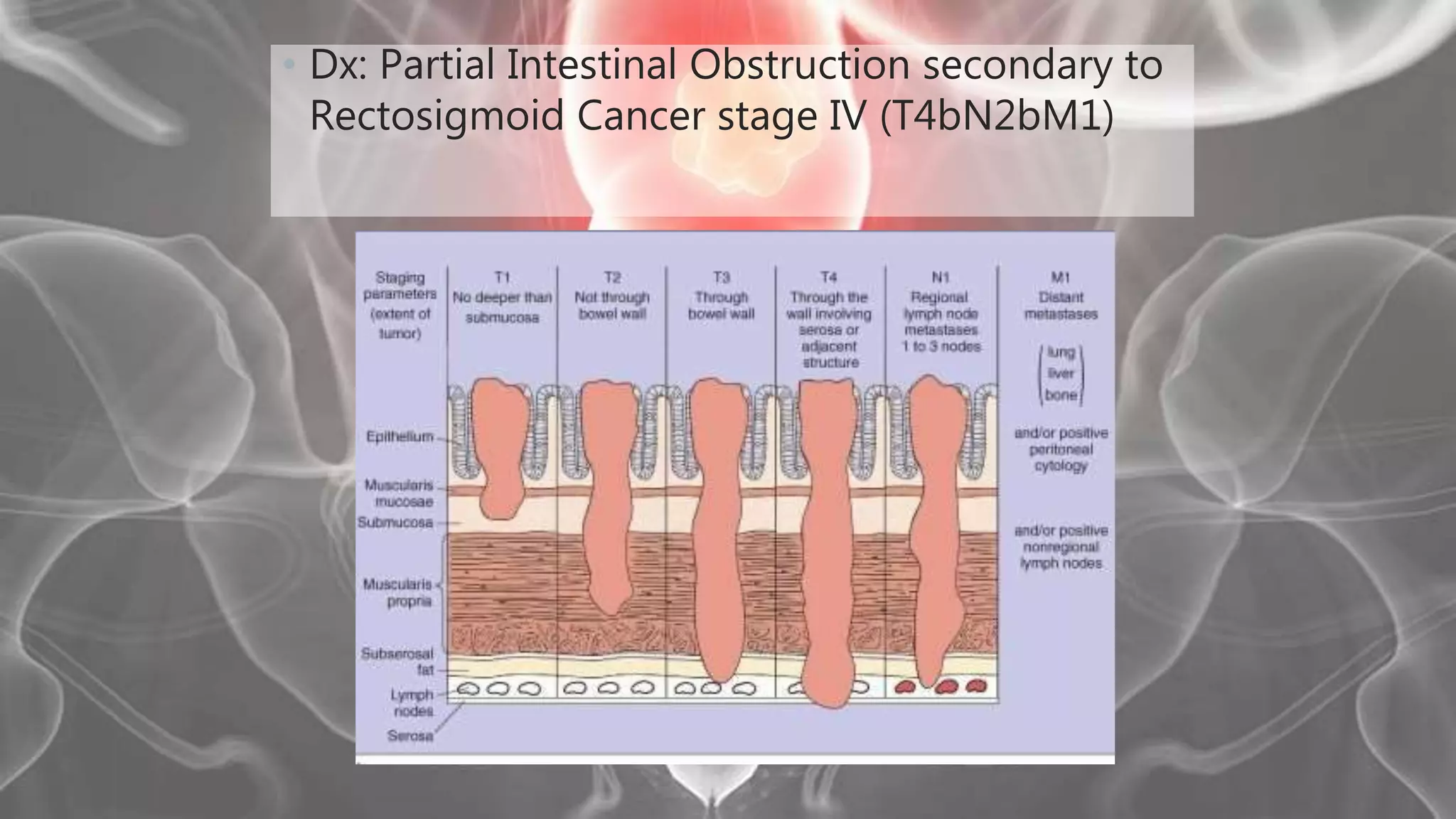













(1) The patient is a 75-year-old female who presented with left lower quadrant pain, decreased bowel movements, weight loss, and recent vomiting of coffee ground material. (2) Physical exam revealed abdominal tenderness and a palpable mass in the left lower quadrant. (3) Imaging showed features suggestive of a colorectal mass. (4) During surgery, a rectosigmoid mass was found involving nearby structures, consistent with stage IV rectal cancer. (5) The patient underwent a Hartmann's procedure and ileostomy for palliation of bowel obstruction from metastatic rectal cancer.





















































































