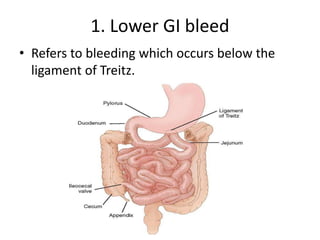
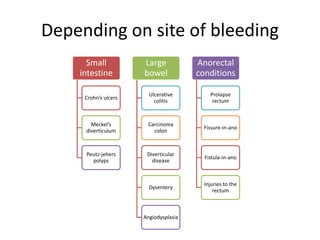
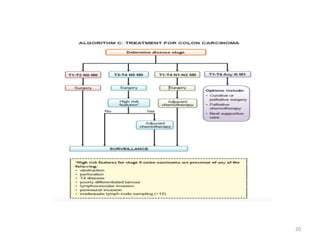
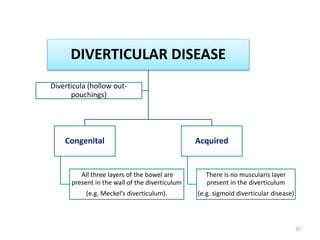
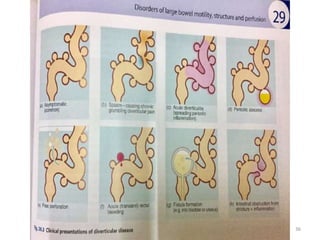
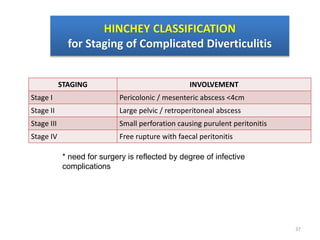
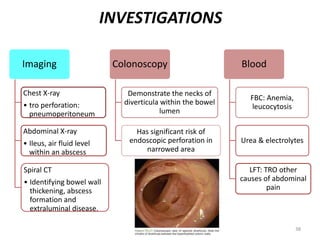
This document provides an outline on lower gastrointestinal bleeding and colorectal diseases. It discusses lower GI bleed, colorectal cancer, inflammatory conditions like diverticular disease, and perianal diseases. For colorectal cancer, it covers epidemiology, pathology, staging, risk factors, investigations, surgery, and management. For diverticular disease, it discusses pathogenesis, clinical features, complications based on Hinchey classification, investigations, and conservative management. The document is a comprehensive reference for lower GI conditions.