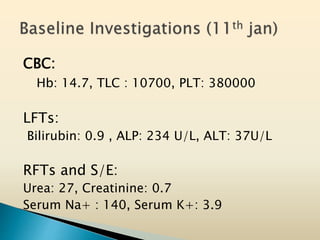
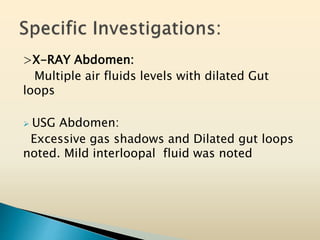
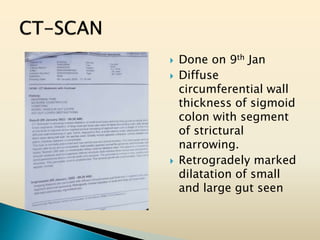
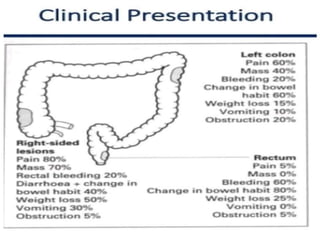
Tasleem Akhtar, a 50-year old female, presented with post-prandial vomiting, abdominal pain, and constipation. Imaging showed signs of intestinal obstruction. She underwent exploratory laparotomy, which found a stricture in the sigmoid colon due to a hard mass. A segment of the sigmoid colon was resected along with the mass. Histopathology revealed colorectal cancer. She was diagnosed with colorectal cancer affecting the sigmoid colon.





















































![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)















