Downloaded 20 times
















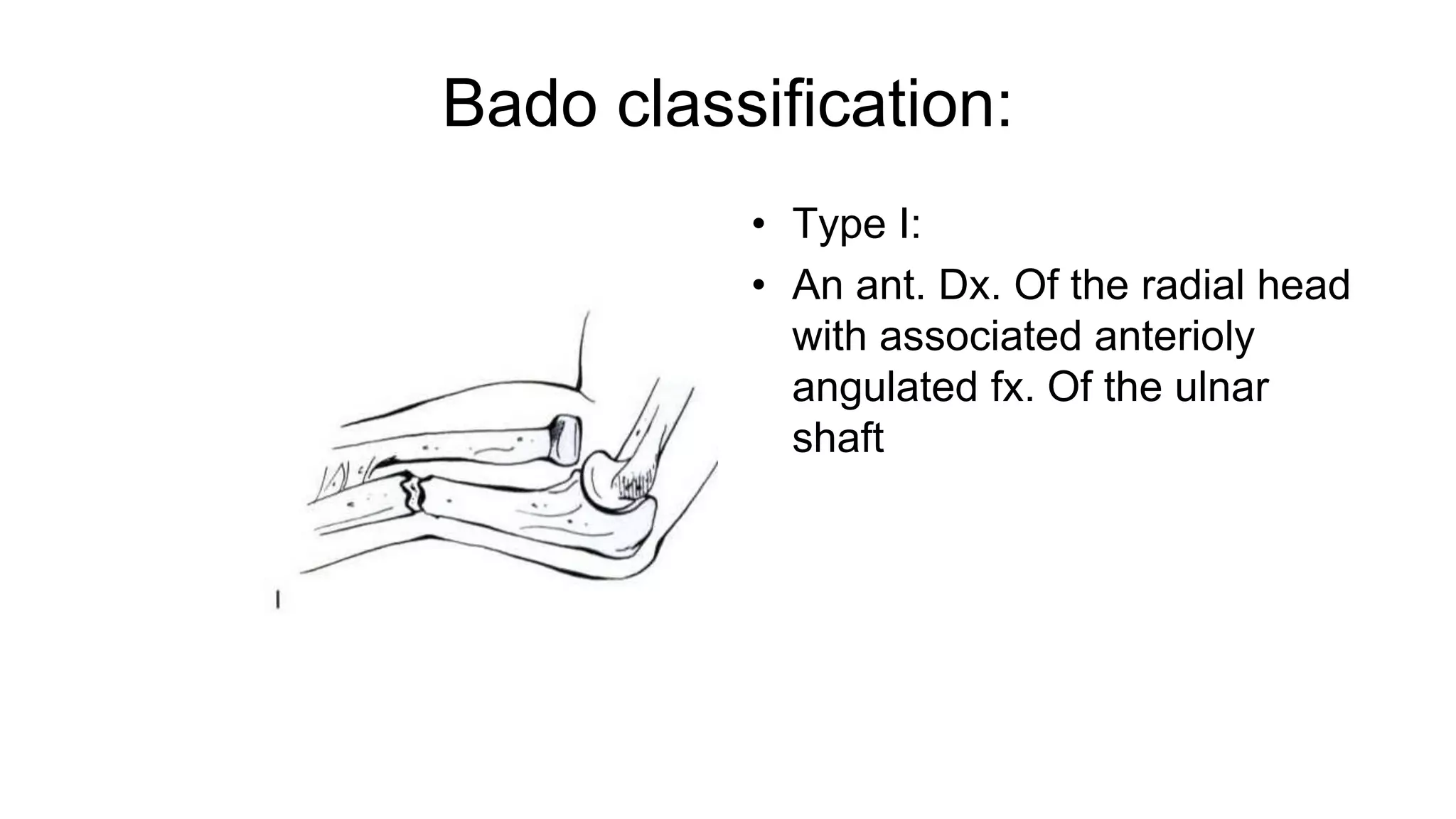

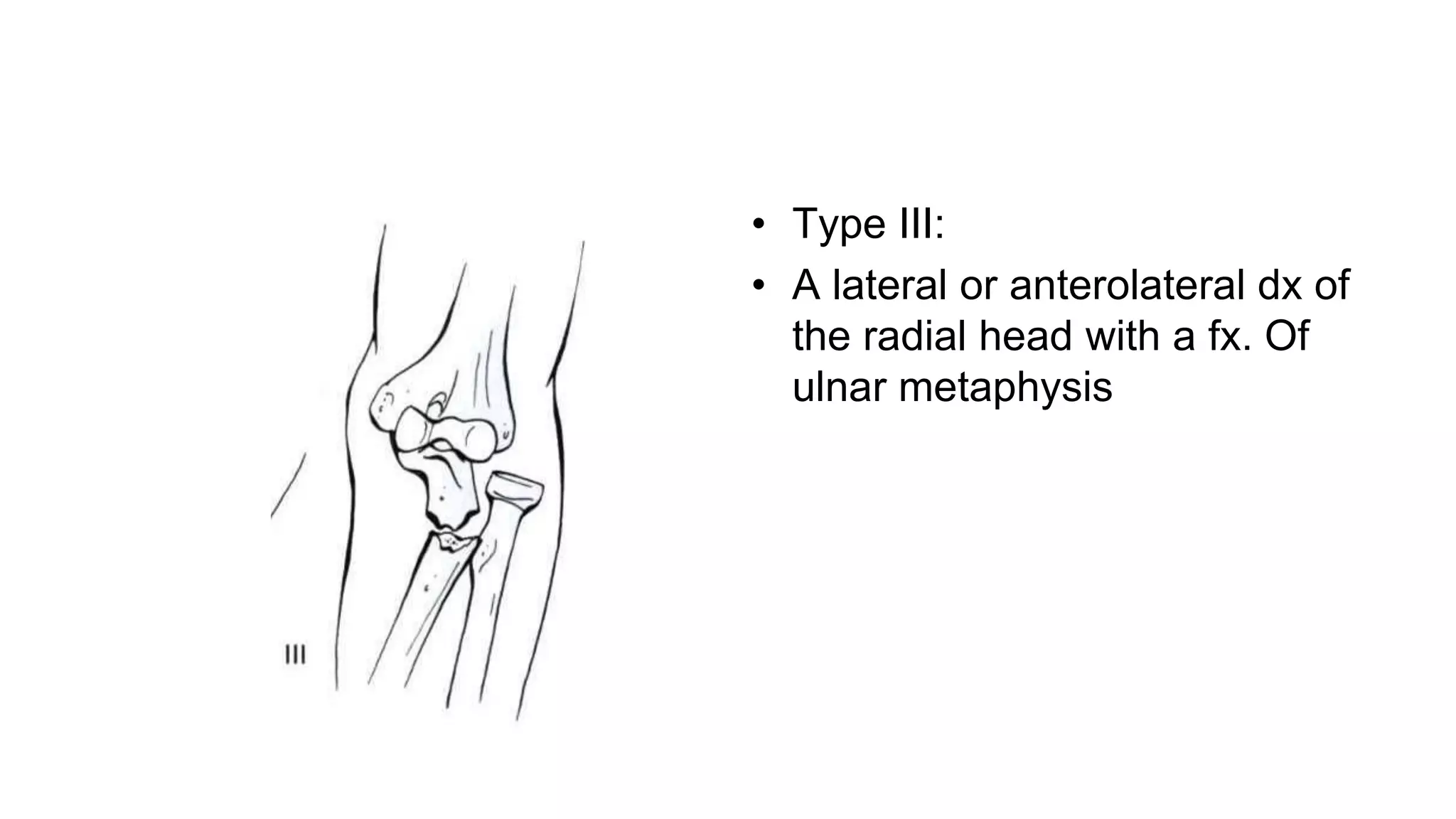
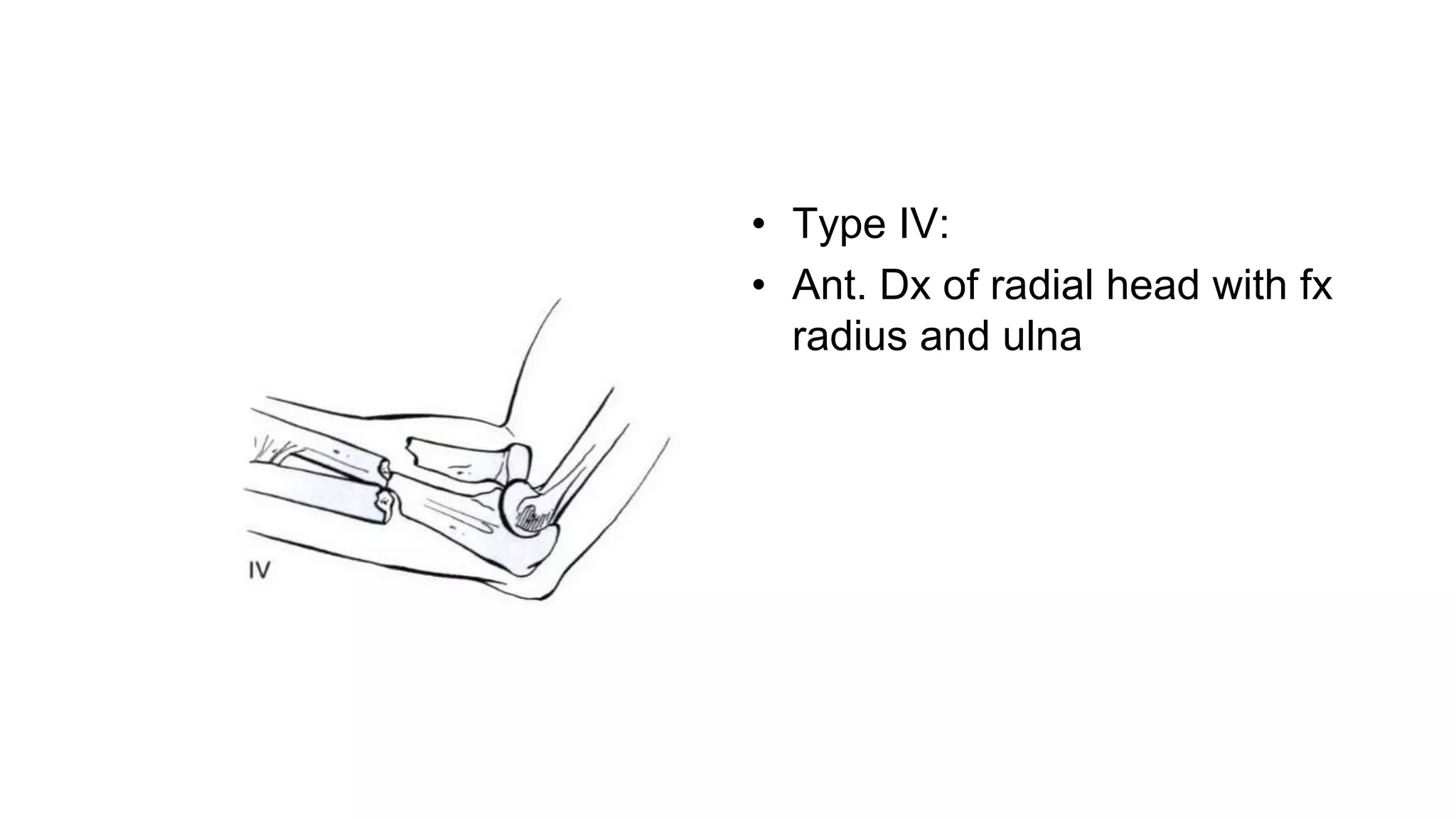



























Fractures of the radius and ulna shafts are common injuries that can have varying classifications and treatment approaches. The document discusses: 1) Classification systems for these fractures including the OTA system that categorizes fractures as Types A, B, or C based on fracture pattern and involvement of one or both bones. 2) Specific fracture types like Monteggia and Galeazzi fractures which involve fractures of the ulna or radius with dislocations of the proximal radioulnar joint. 3) Treatment options including nonoperative management for nondisplaced fractures or operative treatment with external fixation, intramedullary nailing, or plate osteosynthesis depending on the fracture. Complications are also reviewed























































































