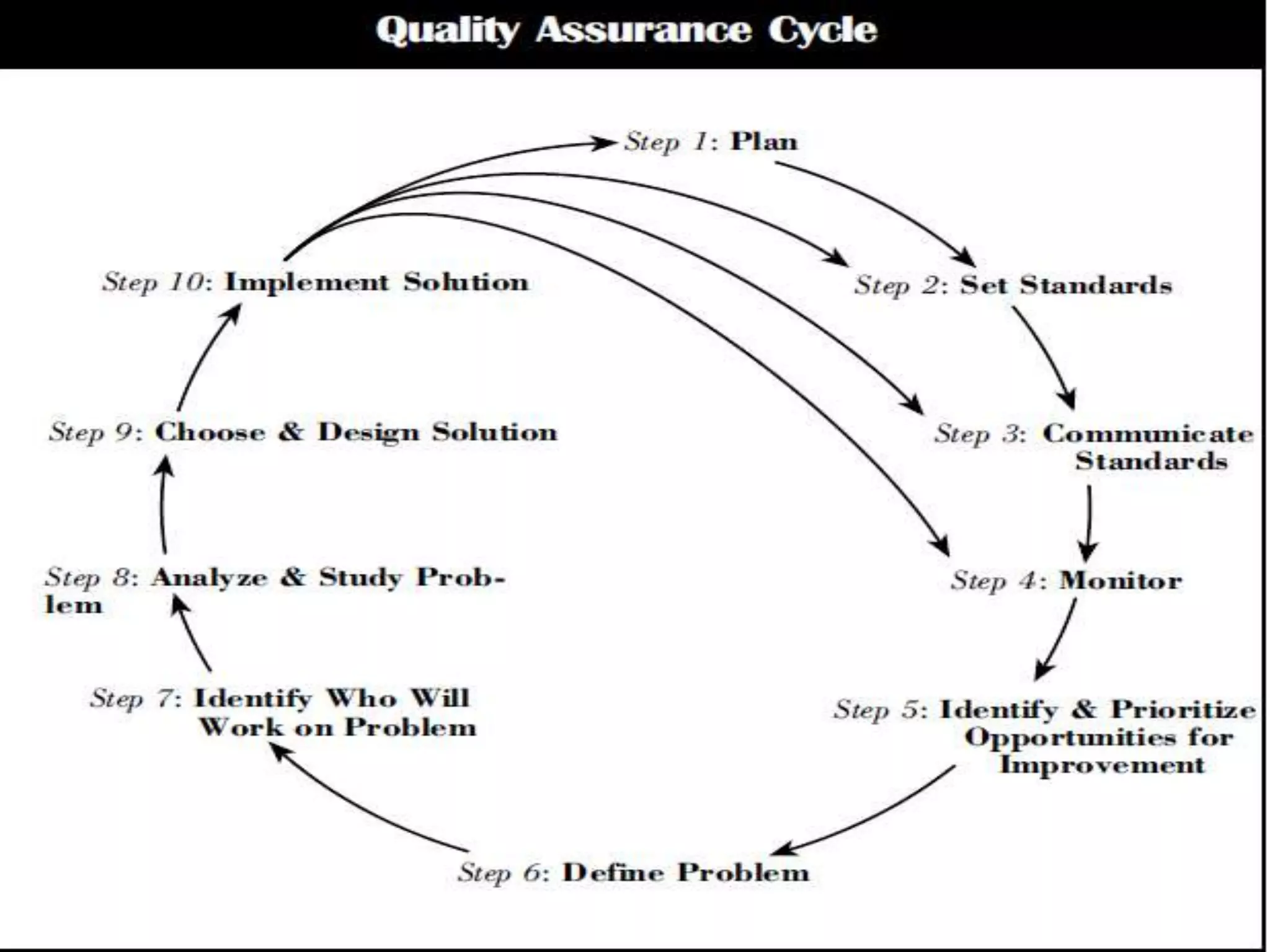
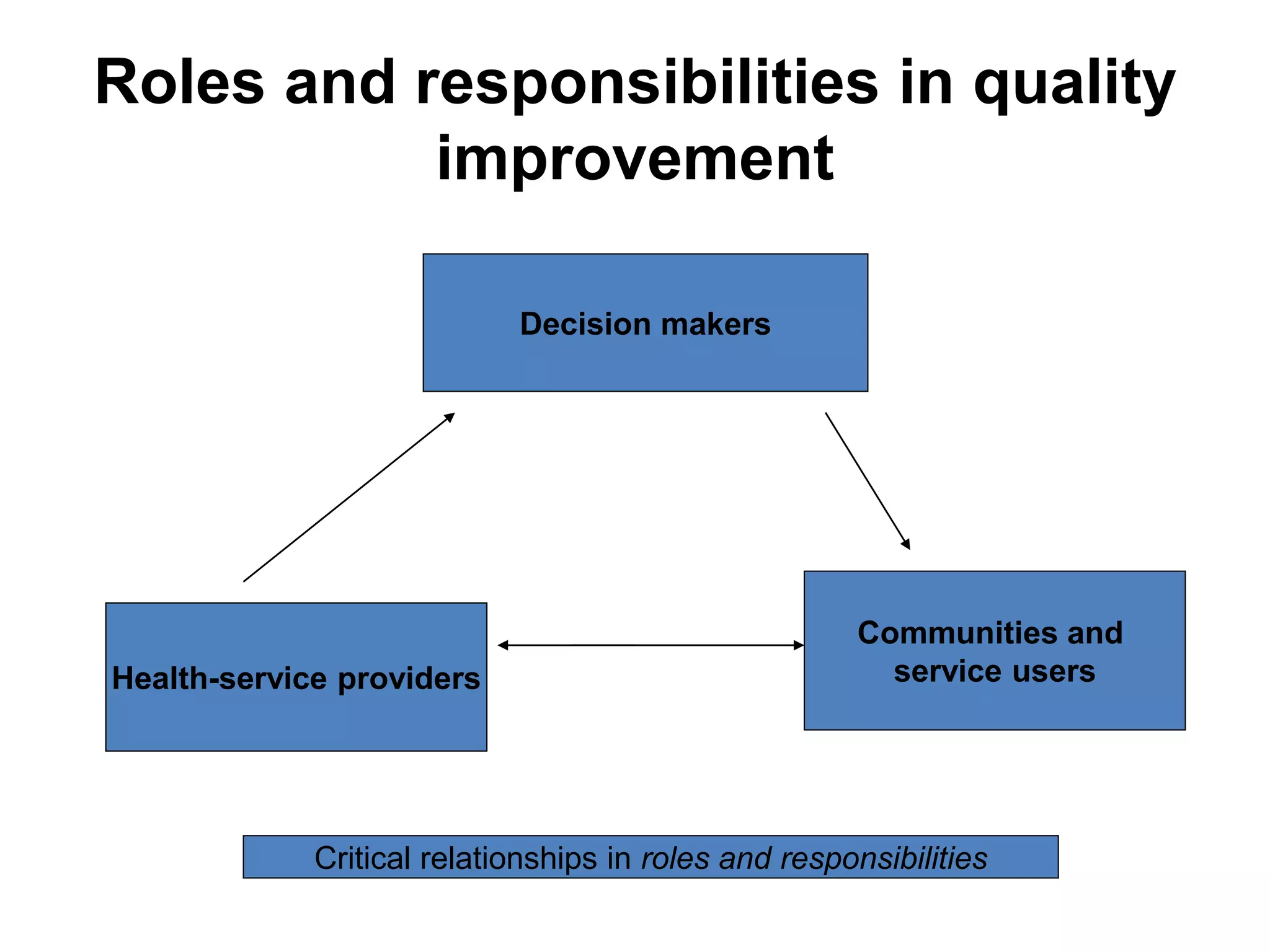
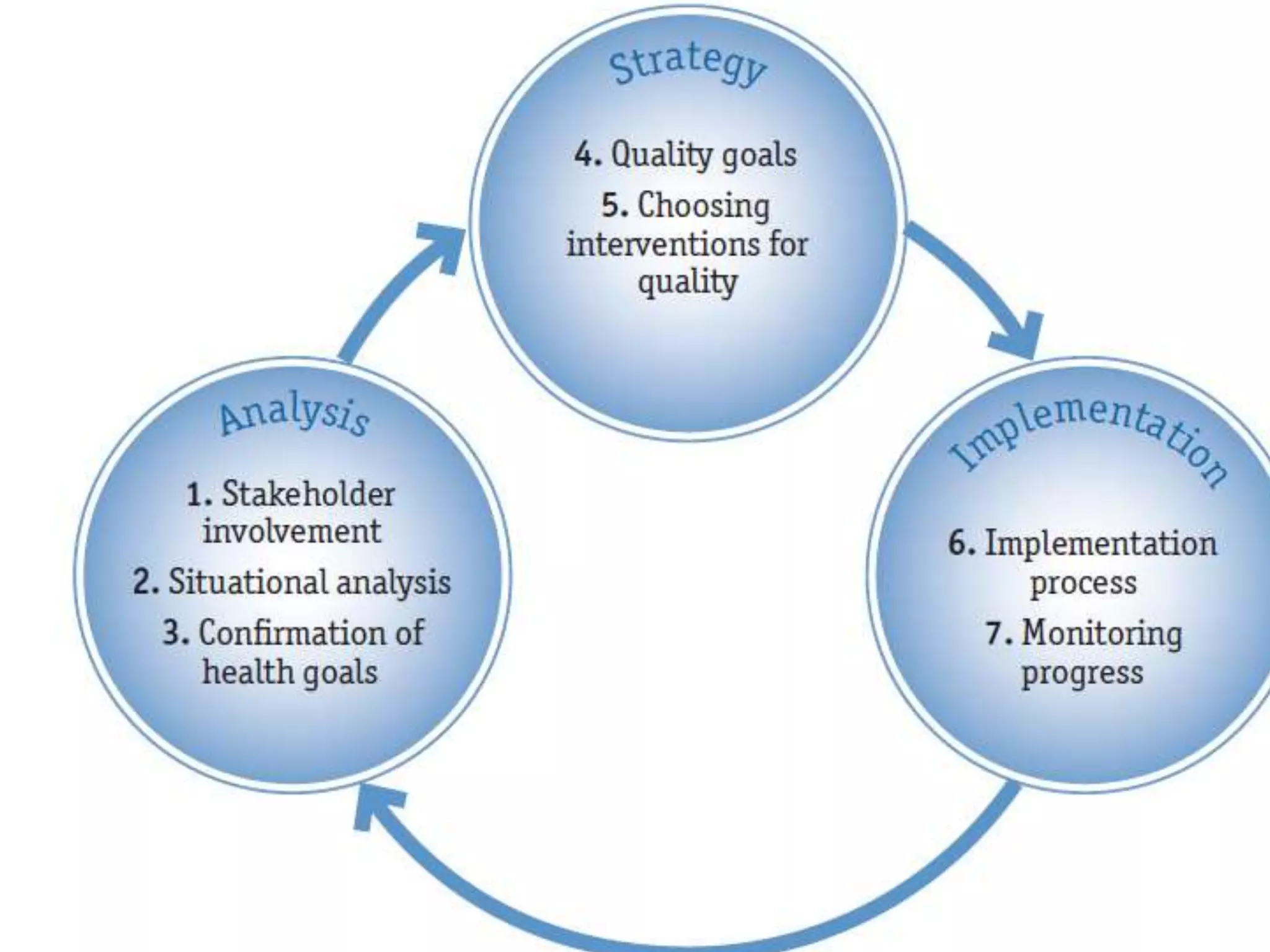
This document discusses various quality processes and concepts including quality assurance, quality control, quality improvement, and total quality management. It defines each concept and describes the relationships between them. Quality assurance involves ensuring compliance to standards, quality control measures actual performance against expected standards, and quality improvement is a structured process to identify and implement improvements. Total quality management incorporates all these approaches and emphasizes continuous improvement through teamwork and a focus on customer needs. The document also outlines the key steps in a quality assurance cycle and roles/responsibilities of different stakeholders in quality improvement.