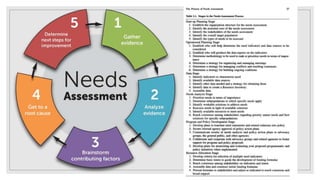
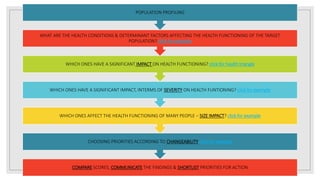
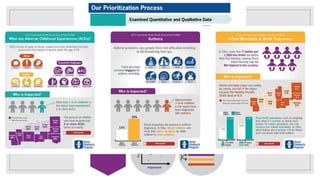
This document outlines the 5 step process for conducting a needs assessment in public health care: 1) Getting Started, 2) Identifying Health Priorities, 3) Assessing Health Priorities, 4) Planning for Change, and 5) Moving On/Reviewing. The goals of needs assessment are to understand the health issues facing a population and agree on priorities and resource allocation to improve health and reduce inequalities. Key aspects include defining the target population, gathering data on health conditions and their impacts, selecting priorities based on impact and changeability, and developing an action plan to address priorities through acceptable and feasible interventions.






![health promotion lecture notes 2023[Autosaved].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/healthpromotionlecturenotes2023autosaved-240524204053-9ab2f7a0-thumbnail.jpg?width=640&height=640&fit=bounds)












































![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)








![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)







