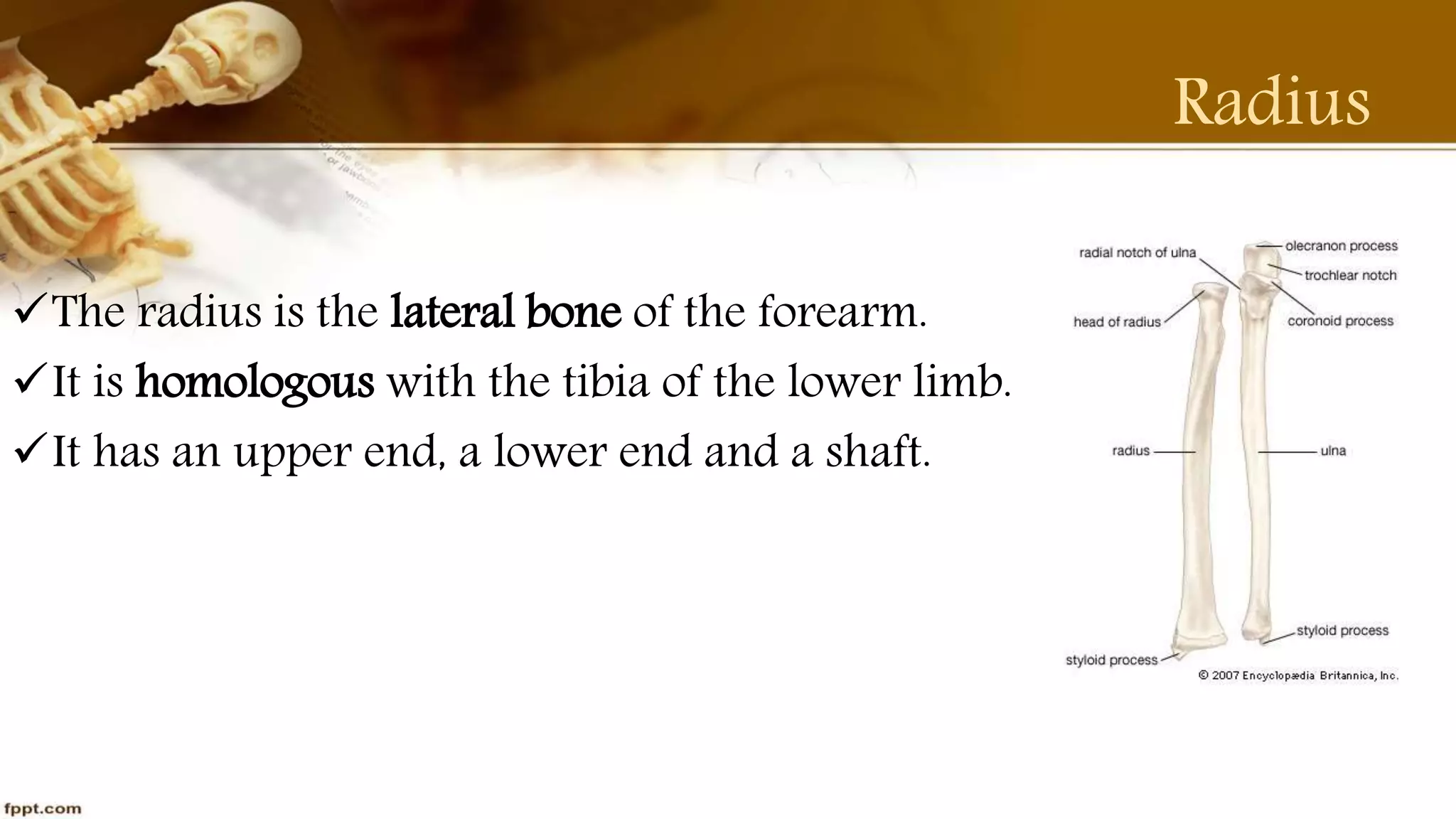
The document provides a detailed overview of the anatomy of the radius and ulna bones in the forearm, including their structure, muscle attachments, and ossification processes. It also discusses clinical conditions such as fractures (Colles's and Smith's fractures), congenital anomalies, and articulation with other bones. Key features of both bones are outlined, highlighting their functions and anatomical relationships.