

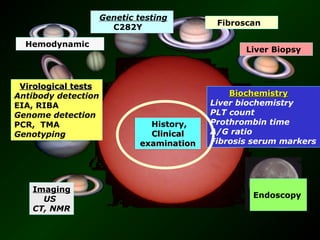
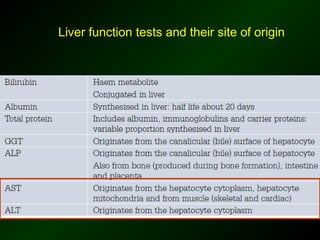
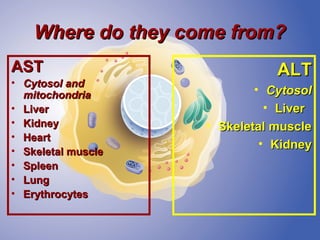
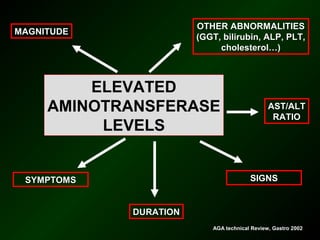
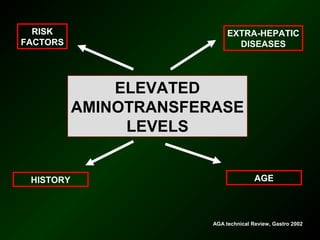
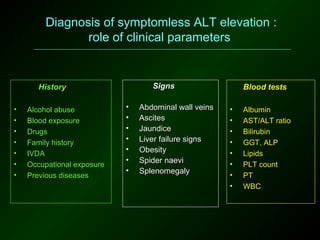
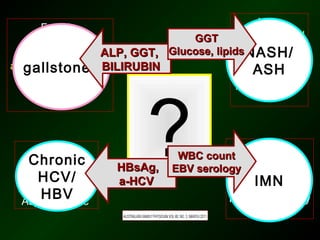
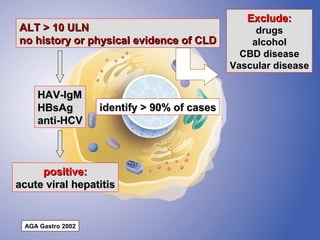
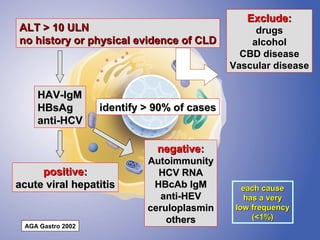
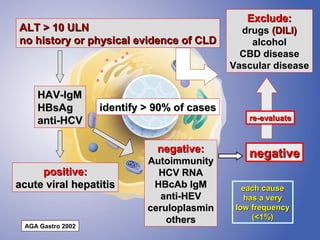
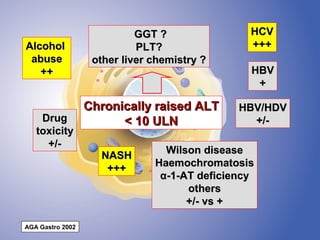
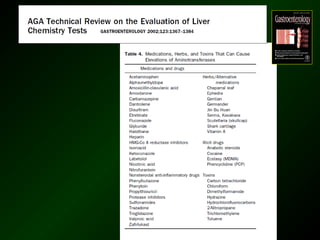

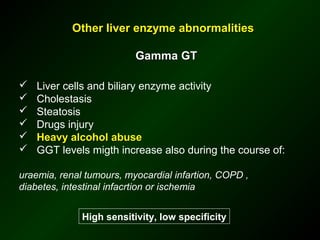
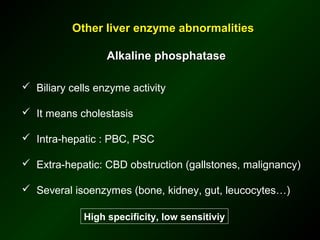

The document discusses diagnostic approaches for liver disease. It outlines three common diagnostic scenarios: 1) a patient referred for clinical symptoms, 2) a patient referred for signs of liver disease, and 3) a patient found to have abnormal liver enzymes incidentally. It then reviews various causes of liver disease including viruses, autoimmunity, and other etiologies. Key diagnostic tests are outlined including imaging, biopsy, virological tests, and genetic testing. Liver enzymes are discussed in depth including their origin and interpretation of abnormal values.




























































































![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)




![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)









