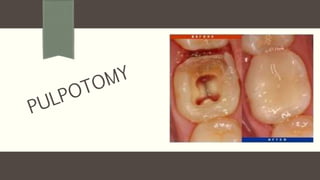
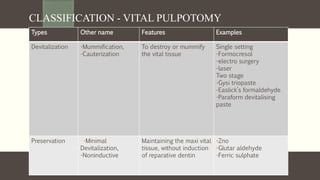
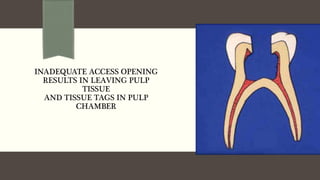
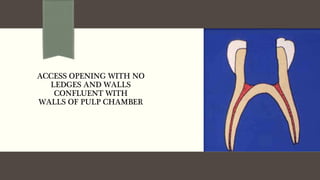
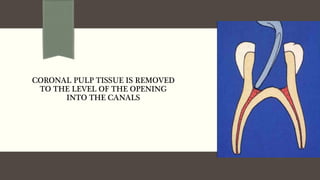
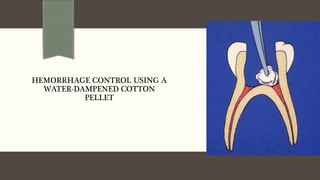
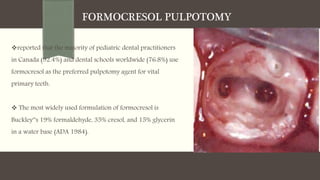
This document discusses various pulpotomy procedures for primary teeth. It defines pulpotomy as removing the coronal pulp and placing a medicament on the radicular pulp stumps. Several materials used for pulpotomy are discussed, including formocresol, glutaraldehyde, calcium hydroxide, ferric sulfate, and MTA. The procedure, success rates, advantages and disadvantages of different materials are summarized. Alternative methods like laser pulpotomy and electrosurgery are also mentioned.


![FORMOCRESOL PULPOTOMY
Formocresol - Buckley [1904]
Sweet – 1930 - Formulated multivisit technique
Doyle – 1962 - Advocated 2 sitting procedure [ complete
devitalization ]
Spedding [ 1965 ] - Gave 5 min protocol partial devitalization
Venham – 1967 - Proposed 15 sec procedure
Current concept uses 4 min of application time](https://image.slidesharecdn.com/pulpotomy-210319053518/85/Pulpotomy-27-320.jpg)





![TECHNIQUE – [1ST VISIT]
LA, excavate caries,
Incorporate paraformaldehyde
and place it on pulp exposure
and seal for 1- 2weeks
Formaldehyde gass liberated
from paraformaldehyde enters
coronal and radicular pulp and
fixes tissue](https://image.slidesharecdn.com/pulpotomy-210319053518/85/Pulpotomy-67-320.jpg)