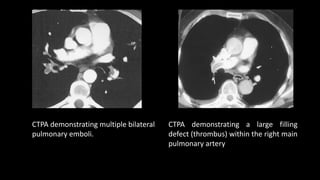
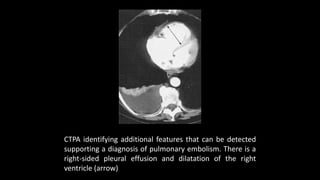
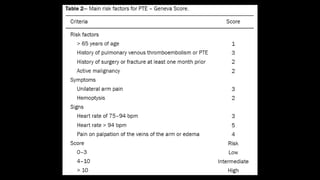
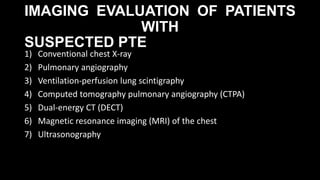
Pulmonary embolism (PE) occurs when a blood clot lodges in the pulmonary arteries. It can be difficult to diagnose due to non-specific symptoms. Imaging plays a key role in the evaluation of suspected PE. Computed tomography pulmonary angiography (CTPA) has become the initial imaging test of choice since it can directly visualize thrombi and rule out other potential causes. It has high sensitivity and specificity. Ventilation-perfusion scintigraphy and pulmonary angiography are older modalities that remain useful in certain settings. New techniques like dual-energy CT may improve detection of subsegmental emboli. Right heart strain on CT suggests worse prognosis.


![Ventilation-perfusion lung
scintigraphy
• Although CTPA is the current gold standard, VQ scan is preferred,
particularly renal failure, contrast material allergies, young females, and
patients who cannot fit into the CT scanner.
• VQ scan has 50-fold lower radiation dose to the breast (0.28–0.9 vs. 50–80
mSv in 64 slice CT) , which makes it useful in young females, including
those who are pregnant.
• Ventilation agents
• aerosolized technetium-99m (Tc-99m) labeled agents [diethylene-
triamine-penta-acetic acid (DTPA), sulfur colloid, and ultrafine carbon
suspensions] and
• radioactive noble gases [Krypton-81m and Xenon-133
• Perfusion portion is performed following the intravenous injection of
200,000–700,000 particles of Tc-99m labeled macro-aggregated albumin
(MAA).](https://image.slidesharecdn.com/pulmonaryembolismimaging-190505165517-200206075248/85/Pulmonaryembolismimaging-190505165517-23-320.jpg)
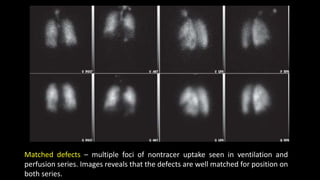
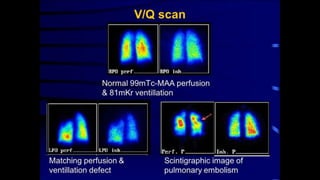
![Normal V/Q study
Ventilation [v] images on top row and perfusion [p] images beneath.
No defects are seen in either series.](https://image.slidesharecdn.com/pulmonaryembolismimaging-190505165517-200206075248/85/Pulmonaryembolismimaging-190505165517-31-320.jpg)