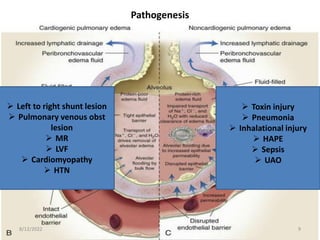
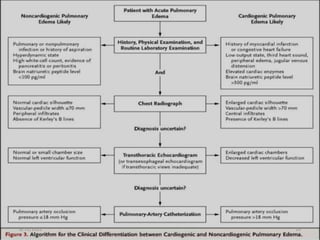
This document provides an overview of pulmonary edema in children, including definitions, classifications, pathogenesis, clinical manifestations, diagnosis, management, and prognosis. Pulmonary edema can be cardiogenic, caused by elevated pressures in the heart, or non-cardiogenic (ARDS). Common causes in children include pneumonia, sepsis, and congestive heart failure. Symptoms include fast breathing and cough. Chest x-rays and BNP levels help diagnose the type. Treatment focuses on oxygen, ventilation if needed, and addressing the underlying cause such as using diuretics, vasodilators, and inotropes for cardiogenic edema. Outcomes depend on the severity of the primary condition but ARDS mortality can be over 50% without treatment.






































































![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)







![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)




