

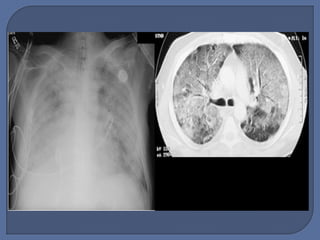

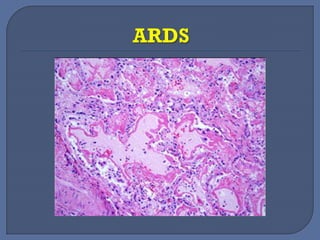






































This document discusses the pathophysiology and management of acute respiratory distress syndrome (ARDS). It notes that ARDS is characterized by pulmonary edema due to increased capillary permeability. Conservative fluid strategies aiming for zero balance can improve outcomes in ARDS patients without shock by reducing pulmonary pressures and edema. A biphasic approach starting with liberal fluids then transitioning to conservative is recommended as hemodynamics stabilize. Diuretics, fluid restriction, and potentially beta-2 agonists or albumin with furosemide in hypoproteinemic patients may help resolve edema. Central pressures, weight, fluid balance, and extravascular lung water should be monitored.