Downloaded 1,310 times
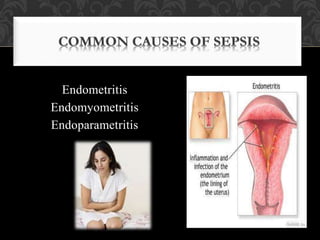
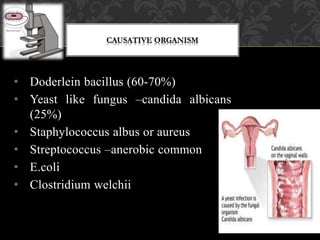

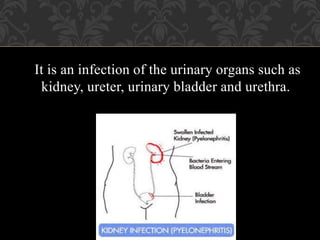


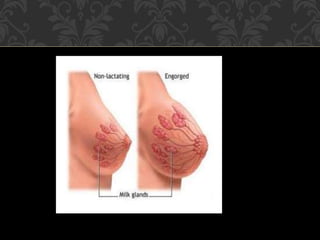

This document discusses several abnormalities that can occur during the postpartum period, known as the puerperium. It defines puerperal pyrexia as a temperature over 100°F occurring on two occasions within the first 10 days postpartum. Puerperal sepsis is defined as an infection of the genital tract occurring as a complication of delivery. Common causes of infection include bacteria like Staphylococcus and Streptococcus. Risk factors, signs and symptoms, treatments and management strategies are described for various postpartum infections and other issues like subinvolution, urinary tract infection, breast engorgement, and cracked nipples.











































































































