Downloaded 637 times













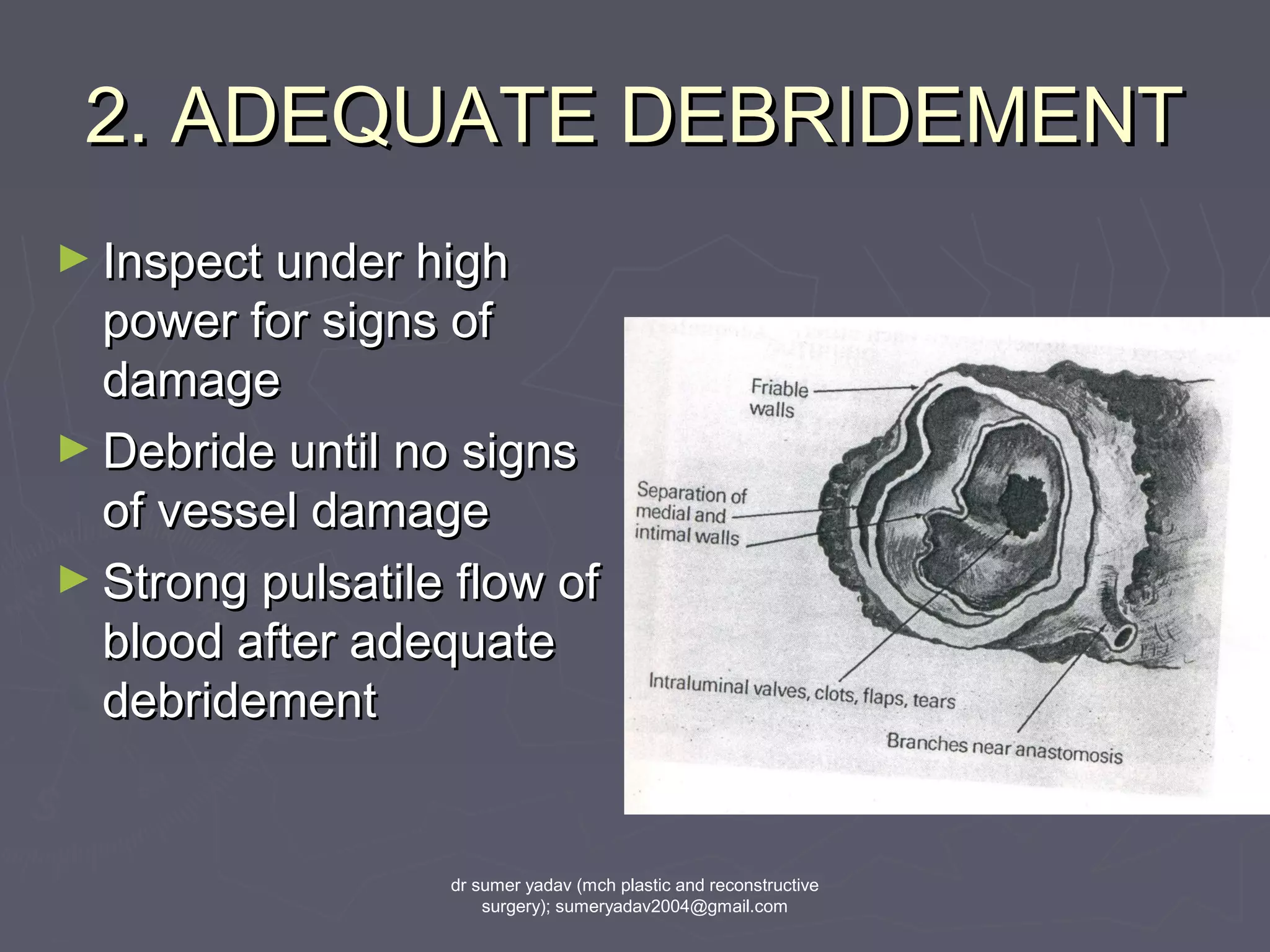


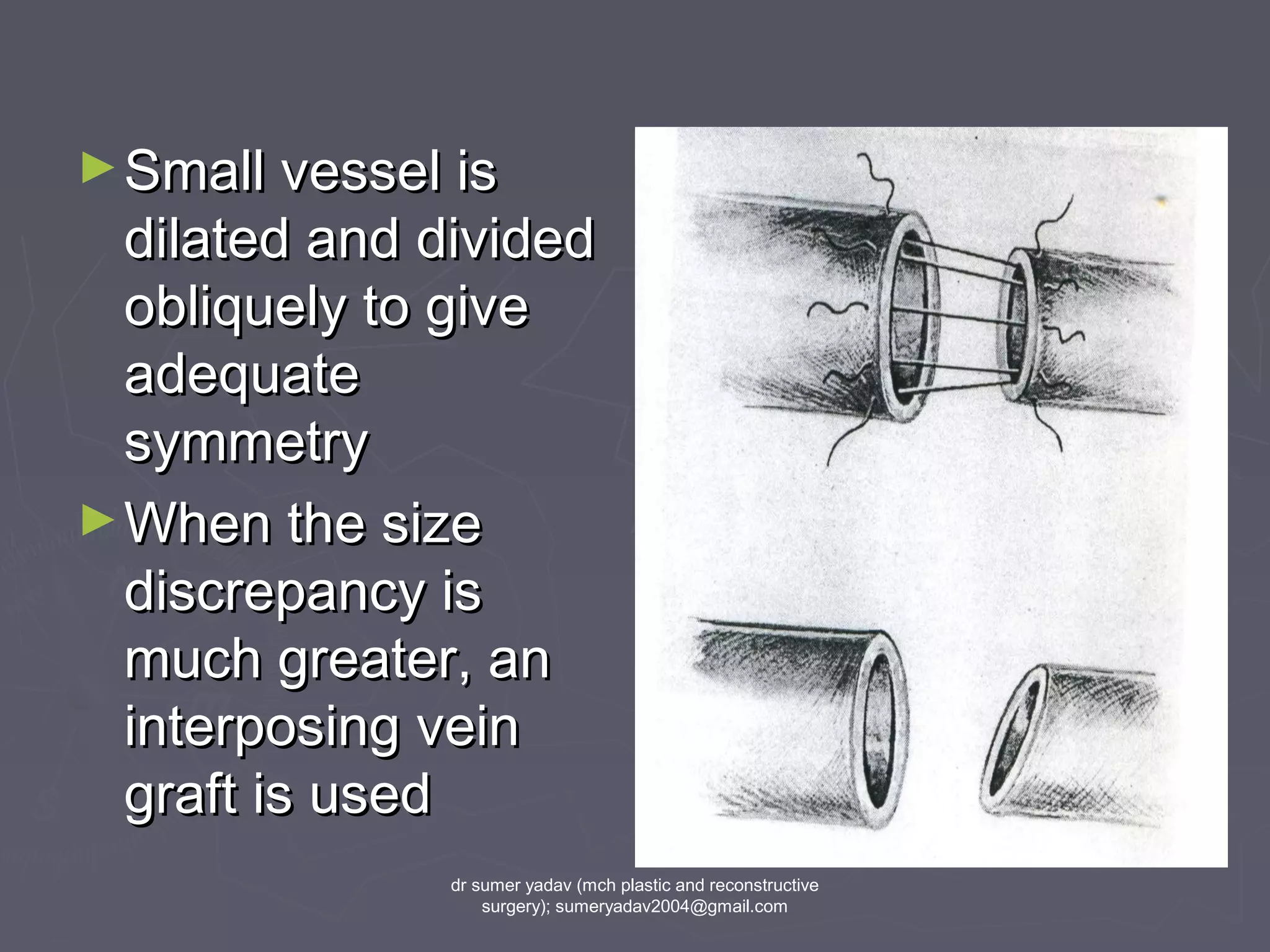









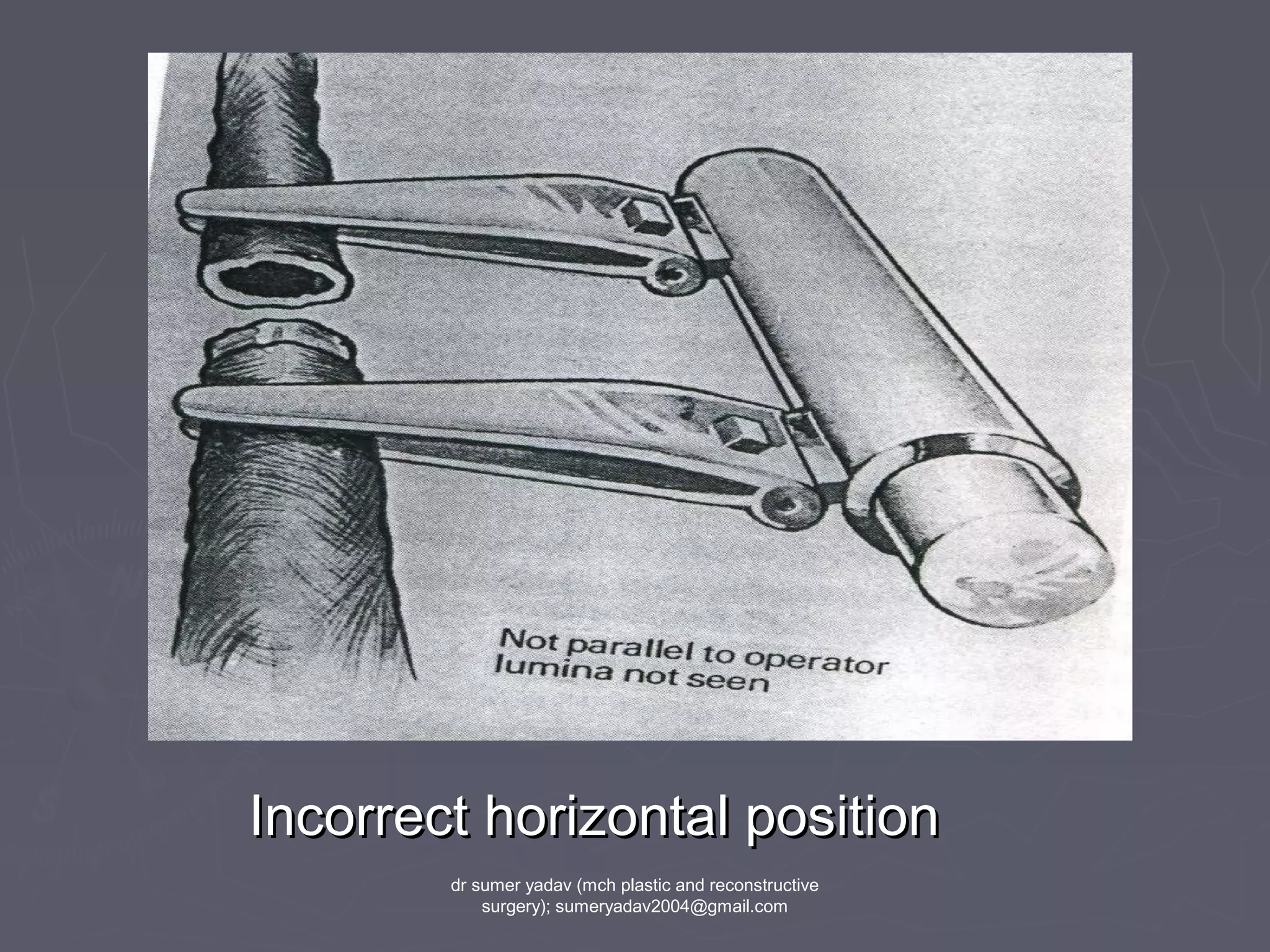

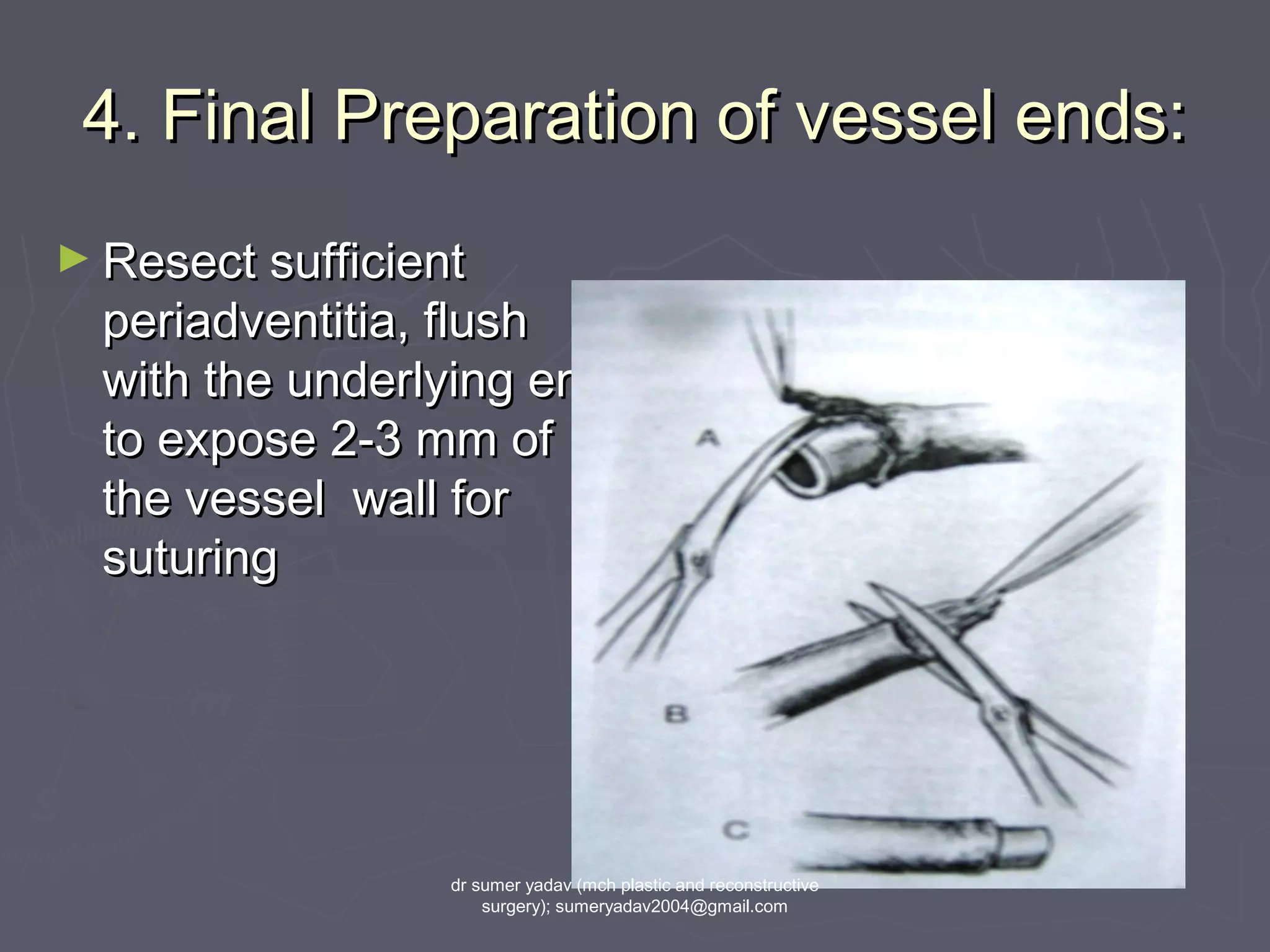



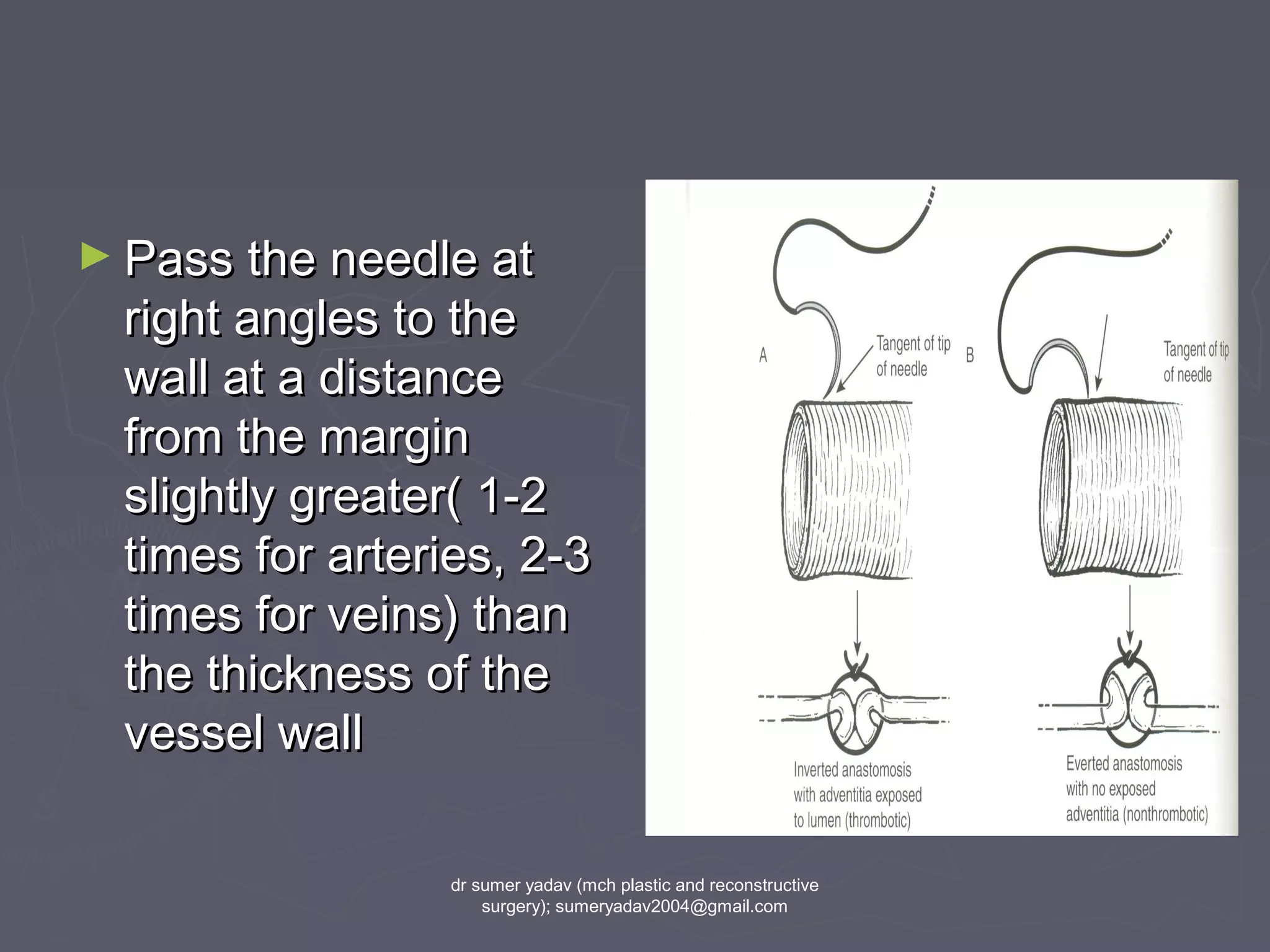

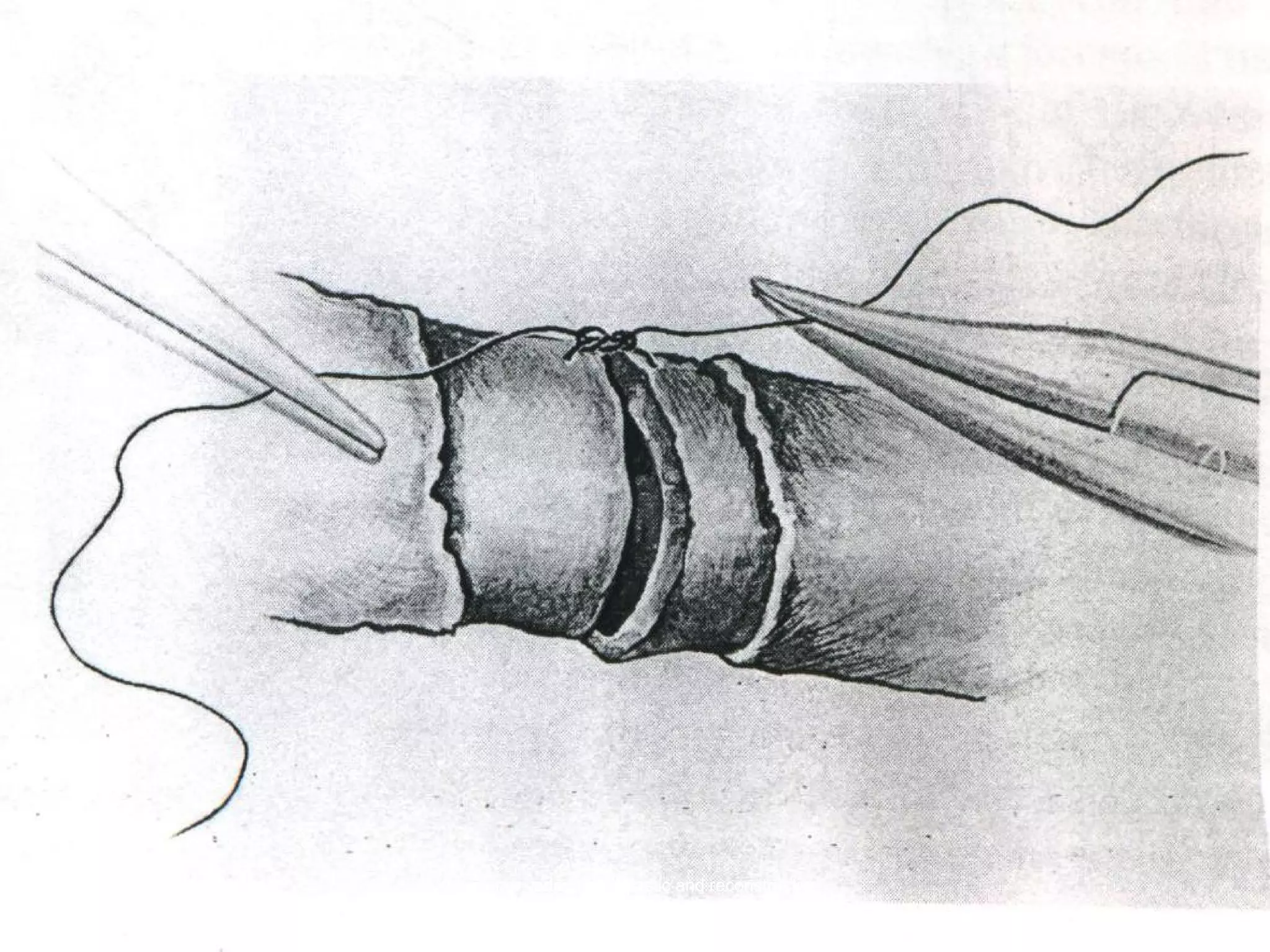
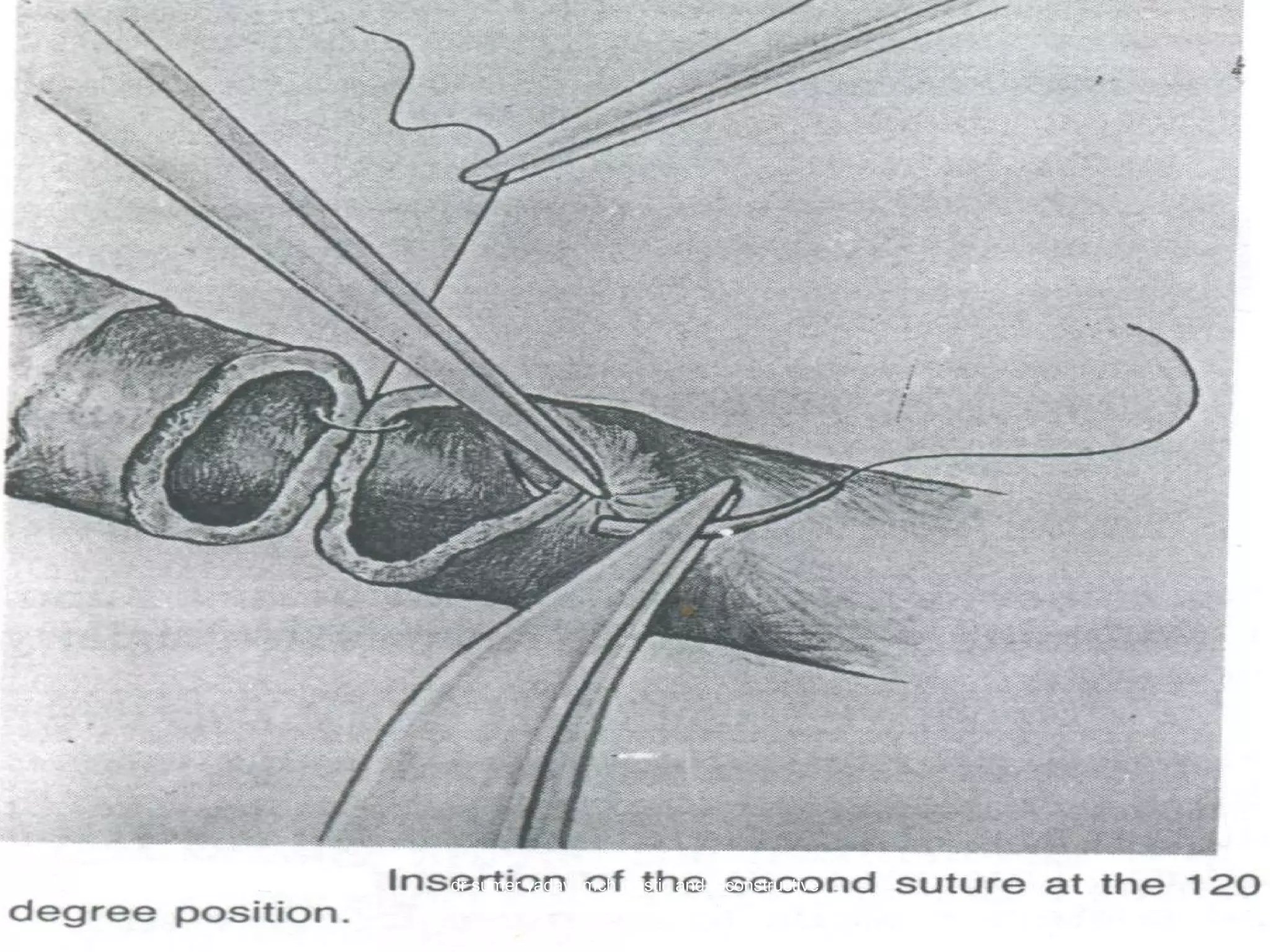



















This document discusses the principles of microvascular surgery. It begins with an introduction to microsurgery and reconstructive microsurgery. The history of microsurgery is then outlined, including important early developments like the invention of the compound microscope and the first vascular anastomosis. The key tools used in microsurgery like the surgical microscope, microinstruments, and microsutures are described. The basic principles of microsurgery are discussed, such as gentle tissue handling and ensuring tension-free anastomoses. Details are provided on vessel preparation, dissection techniques, and the technique of performing an anastomosis.