Student's elbow, or 'Olecranon Bursitis' is a condition where a small sack of tissue over the tip of your elbow becomes inflamed and swollen. The pointy bit of bone at the end of your elbow is called the 'olecranon' and the small sack which sits between the bone and the skin is called a 'bursa'.
Bhaskar Health News and Medical Education is leading source for trustworthy health, medical, science and technology news and information. Providing world health information Medical Education.
Bhaskar Health News and Medical Education is dedicated to medical students, physiotherapists, doctors, nurses, paramedics, physician associates, dentists, pharmacists, midwives and other healthcare professionals.
We're committed to being your source for expert health guidance. Bhaskar Health and Medical Education.
Source : https://www.bhaskarhealth.com
Health Shop: https://www.bhaskarhealth.org
@drrohitbhaskar @bhaskarhealth
#DrRohitBhaskar #BhaskarHealth
#Health #Medical #News #Physiotherapy
Student's elbow, or 'Olecranon Bursitis' is a condition where a small sack of tissue over the tip of your elbow becomes inflamed and swollen. The pointy bit of bone at the end of your elbow is called the 'olecranon' and the small sack which sits between the bone and the skin is called a 'bursa'.
Bhaskar Health News and Medical Education is leading source for trustworthy health, medical, science and technology news and information. Providing world health information Medical Education.
Bhaskar Health News and Medical Education is dedicated to medical students, physiotherapists, doctors, nurses, paramedics, physician associates, dentists, pharmacists, midwives and other healthcare professionals.
We're committed to being your source for expert health guidance. Bhaskar Health and Medical Education.
Source : https://www.bhaskarhealth.com
Health Shop: https://www.bhaskarhealth.org
@drrohitbhaskar @bhaskarhealth
#DrRohitBhaskar #BhaskarHealth
#Health #Medical #News #Physiotherapy
The basis of manual small incision cataract surgery is the tunnel construction for entry to the anterior chamber.
The parameters important for the structural integrity of the tunnel are the self-sealing property of the tunnel, the location of the wound on the sclera with respect to the limbus, and the shape of the wound.
Cataract surgery has gone beyond just being a means to get the lens out of the eye.
Postoperative astigmatism plays an important role in the evaluation of final outcome of surgery. Astigmatic consideration, hence, forms an integral part of incisional considerations prior to surgery.
Osteoarthritis knee- introduction and approachJoe Antony
Osteoarthritis (OA) of the knee is a degenerative joint disorder characterized by structural changes like cartilage loss, synovial inflammation, and bone remodeling . Knee OA commonly affects daily activities due to symptoms like joint pain and stiffness, impacting functional abilities . Various factors contribute to knee OA development, including mechanical, enzymatic, and biological factors . In knee OA patients, proinflammatory cytokines like IL-6 and TNF-α have been found to correlate with functional impairment assessed by WOMAC scores, indicating a potential impact on knee joint function . Understanding the interplay between aging and knee OA is crucial, as aging processes can exacerbate the degenerative changes in the knee joint, leading to functional limitations . Evaluating patients' perspectives on knee OA management through instruments like the Knee Outcome Survey Activity Daily Living Scale (KOS-ADLS) is essential for assessing the success of interventions
Gait deviations in Transtibial prosthesis usersJoe Antony
Gait deviations in transtibial amputations involve altered biomechanics and asymmetries. Research highlights that spatiotemporal gait parameters are affected, with reduced propulsive force, knee extension moment, and increased knee abduction moment in the amputated leg. Additionally, individuals with transtibial amputations exhibit shorter stance times, longer swing times, and larger step lengths compared to able-bodied individuals. These deviations can lead to asymmetrical loads, potentially causing issues like osteoarthritis or lower back pain. Furthermore, gait asymmetry in transtibial amputees is associated with poor functional outcomes, impacting performance-based physical function tests like the Timed Up and Go, the 10-Meter Walk Test, and the 6-Minute Walk Test. Understanding these gait abnormalities is crucial for tailored interventions and prosthetic design to improve outcomes for individuals with transtibial amputations.
Basics of electro myo graphy study (EMG)Joe Antony
Electromyography (EMG) is a vital technique in the field of bioelectrical signal analysis. It involves capturing muscle activity through surface or needle electrodes for diagnostic purposes. EMG signals can be analyzed to detect various muscle conditions, such as myopathic or neuropathic lesions, using numerical parameters. The spatial frequency bandwidth of surface EMG signals is crucial for detailed muscle activity reconstruction, with appropriate inter-electrode distances being essential for accurate mapping. In the context of neuro-monitoring, EMG plays a role in intra-operative detection of adverse events and predicting postoperative outcomes, especially when used complementarily with other modalities like motor evoked potentials. Overall, EMG serves as a valuable tool for understanding muscle function, diagnosing muscle disorders, and enhancing neuro-monitoring practices
Principles of tendon transfer surgeries in rehabilitationJoe Antony
Tendon transfers, a fundamental aspect of reconstructive surgery, represent a sophisticated intervention in the domain of orthopedics and plastic surgery. This intricate procedure involves the repositioning or redirection of tendons to restore lost function, correct deformities, or alleviate debilitating conditions resulting from tendon injuries, neurological disorders, or musculoskeletal anomalies. By harnessing the body's inherent capacity for adaptation and regeneration, tendon transfers offer a transformative solution to patients grappling with impairments affecting mobility, dexterity, and overall quality of life.
Within the realm of medical science, tendon transfers stand as a testament to the innovative intersection of anatomy, biomechanics, and surgical expertise. Guided by meticulous anatomical knowledge and informed by patient-specific considerations, surgeons meticulously navigate the intricate network of tendinous structures to achieve optimal outcomes. This precise manipulation of tendons demands not only technical proficiency but also a profound understanding of functional anatomy, pathological processes, and the dynamic interplay between muscles and joints.
The rationale underlying tendon transfers rests upon the principle of functional restoration through strategic tendon re-routing. Whether addressing paralysis resulting from nerve injury or rectifying muscular imbalances precipitated by congenital anomalies, the overarching goal remains consistent: to enhance musculoskeletal function and foster meaningful improvements in patient well-being. By redistributing the forces exerted by muscles across joints, tendon transfers serve as a cornerstone in the rehabilitation arsenal, offering a pathway towards enhanced motor control, stability, and range of motion.
In this discourse, we embark on a comprehensive exploration of tendon transfers, delving into the intricacies of surgical technique, patient selection criteria, rehabilitative protocols, and outcomes assessment. Through a synthesis of clinical insights, scientific inquiry, and empirical evidence, we endeavor to illuminate the multifaceted dimensions of this therapeutic modality. By elucidating the underlying principles and practical applications of tendon transfers, we aspire to equip healthcare practitioners with the requisite knowledge and insights to navigate this dynamic landscape and empower patients with newfound avenues for functional restoration and renewed vitality.
International standards for neurological classification of spinal cordJoe Antony
The International Standards for Neurological Classification of Spinal Cord Injury (ISNCSCI) or more commonly referred to as the ASIA Impairment Scale (AIS), was developed by the American Spinal Injury Association (ASIA) as a universal classification tool for Spinal Cord Injury based on a standardized sensory and motor assessment, with the most recent revised edition published in 2011. The impairment scale involves both a motor and sensory examination to determine the sensory and motor levels for the right and left side, the overall neurological level of the injury and completeness of the injury i.e. whether the injury is complete or incomplete.
Wheelchairs and seating systems allow individuals with mobility impairments to actively participate at home, work, school, and the community. The quality of life of an individual is reflective of the overall effectiveness of the wheelchair and seating system when considering activities of daily living (ADLs). Therefore it is imperative that the multidisciplinary team of rehabilitation professionals
considers not only the individual and the wheelchair but also the
activities, context, policies, and personal assistance associated with the technology. Historically, rehabilitation professionals have
focused on functional mobility at the time of implementation of
the wheelchair and seating system. Now, as a result of changes in the overall health care environment, driven by a need for increased value, rehabilitation professionals must integrate a more holistic
approach to manage costs while improving outcomes at the time
of implementation and throughout the life of the wheelchair and seating systems.To better understand the long-term effects of the wheelchair and seating system and to maximize the functional
outcomes of the individual, rehabilitation professionals across the multidisciplinary health care team must understand the advances in current technology as well as best practices in the service delivery.
process. The value of the wheelchair and seating system within
the context of health care now extends beyond the four walls of a
traditional clinic to the community in which the individual uses
the wheelchair and seating system.
Significant advances in management have resulted in an increase in survival after burn injury in regions of the world with access to current medical and surgical resources. As a consequence, burn survivors with access to up-to-date care and who tend to be young adults have long-term sequelae that impair function and limit
return to preinjury function, including work and community
reintegration. Up to 1 million burns require treatment annually in North America, and over 10 times as many burns occur worldwide. In low-income and middle-income countries, mortality is significantly greater than in high-income countries.The future
of burn care will be challenged by the expense and complexity of treatment, a predicted shortage of qualified burn care providers, and an aging population.
Physical medicine and rehabilitation (PM&R) is a relatively young specialty that developed during the 20th century, with signifi cant growth and development stimulated by
two World Wars and by increasingly severe epidemics of
paralytic poliomyelitis during the fi rst half of the 20th century
(1–4). During and after each of the World Wars, many soldiers returned with serious injuries and severe disabilities, and physicians and therapists were needed to treat and manage their chronic disabling conditions. This was particularly true after World War II, when the availability of antibiotics and improved surgical techniques allowed more injured soldiers to survive, albeit with significant
disabilities. Similarly, over the same time period, increasingly
severe epidemics of polio, frequent industrial accidents,
and escalating motor vehicle accidents as a result of
the increased availability of automobiles and higher-speed
roadways added greatly to the burden of impairment and
disability among the civilian population. Thus, events in the
fi rst half of the 20th century necessitated the development
of new restorative treatment programs incorporating new
physical and rehabilitative techniques, and the establishment
of training programs for physicians and therapists to
administer the treatments.
Nevertheless, with the exception of a relatively few scattered physical medicine physicians, it was not until the second half of the 20th century that specialists in rehabilitation medicine could profi tably direct their energies exclusively, or even preferentially, to rehabilitation outside of the unprecedented and unsustainable circumstances of wartime
military programs. Also largely missing until the second half
of the 20th century were separate departments in academic and nonacademic medical centers devoted to the specialty, established training programs in PM&R, a sufficient number of PM&R practitioners, separate dedicated facilities for
provision of rehabilitation services (e.g., dedicated wards in hospitals or separate rehabilitation centers), forums for the interchange of ideas (e.g., texts, journals, and professional societies), recognition by professional colleagues and the
public that rehabilitation medicine specialists provided a
needed service, and supportive legislation that would provide
fi nancial mechanisms to develop and provide such
resources
In lesions below the mid-pons, a state of flaccidity, termed spinal shock, ensues immediately after injury with loss of all reflexes caudal to the injury.
The resolution of spinal shock occurs gradually , taking weeks to months.
The recovery from spinal shock is poorly understood and likely results from multiple, simultaneous adaptations in spinal processing that allow motor neuron to function independently from supraspinal control.
Existence of spinal shock, followed by a gradual return of reflexes that eventually become hyperactive, suggests that spasticity is not just a result of a simple on/off switch triggered by an alteration in inhibitory and facilitative signals
Walking depends on the repeated performance by the lower limbs of a sequence of motions that simultaneously advances the body along the desired line of progression while also maintaining a stable weight-bearing posture. Effectiveness depends on free joint mobility and muscle action that is selective in both timing and intensity. Normal function is also optimally conservative of physiologic energy. Pathologic conditions alter the mode and efficiency of walking. The loss of some actions necessitates substitution of others if forward progression and stance stability are to be preserved. Through a detailed knowledge of normal function and the types of gait errors that the various pathologic conditions can introduce, the clinician becomes able to define the significant deficits and plan appropriate corrective measures
Tendo Achilles tenotomy as a part of Ponsetti techniqueJoe Antony
Most CTEV children will need the tenotomy, which is a minor procedure usually done
with local anaesthetic. Children need the tenotomy because their heel (Achilles) tendon is short and tight
and it pulls the heel up.If it is not corrected the child will walk on tiptoes. Some doctors use general anaesthetic for older patients. After the tenotomy a final POP cast is applied and left on for three weeks. During this time the tendon regenerates in the lengthened position and the foot
can be bent up easily towards the front of the leg (dorsiflexion). If your baby is unhappy after the tenotomy, it is fine to use some paracetamol
as you would after vaccinations
Prosthetic management of individuals with upper extremity
amputations presents all health professionals, including
prosthetists and therapists, with a set of unique challenges.
For those wearing an upper extremity prosthesis, the terminal
device (TD) of the prosthesis is not covered or obscured
by clothing in the same way that a lower extremity prosthesis
is “hidden” by pants, socks, and shoes. The person with
upper extremity amputation must cope with not only physical
appearance changes, but the loss of some of the most
complex movement patterns and functional activities of
the human body.
In addition, upper extremity limb loss deprives the patient
of an extensive and valuable system of tactile and proprioceptive
inputs that previously provided “feedback” to guide and
refine functional movement. Even the simplest tasks
related to grasp and release become challenging. The ability
to position the prosthetic limb segments in space, as well as
the ability to maintain advantageous postures needed to
manipulate objects, challenge the medical community to
continuously improve the functional and aesthetic outcomes
of prostheses for patients in this population.
Pelvic floor disorders include a wide-ranging group of potentially
disabling, embarrassing, and often painful conditions that can
greatly affect a person’s quality of life. The pelvic floor consists of
muscles, fascia, and ligaments that support the pelvic organs and
help to provide control for bodily functions. Pathology within the
musculoskeletal and neurologic structures of the deep pelvis can
lead to the development of pelvic pain, dyspareunia, voiding dysfunction
including urinary incontinence or urinary urgency, fecal
incontinence (FI), constipation, and pelvic organ prolapse (POP)
.
Both women and men can develop pelvic floor disorders,
although women are at increased risk compared with men because
of their unique anatomy and biomechanics. The female pelvis is
broader and shallower, requiring greater muscular and ligamentous
stiffness to provide support and stability. Women are also
more likely to incur injury to the pelvic floor as a result of pregnancy
and childbirth. As a result, abnormal biomechanics of the
pelvic floor muscles (PFMs) may lead to changes in contraction,
relaxation, muscle strength, and myofascial pain. In a 2014 study,
the prevalence of symptomatic pelvic floor disorders in the United
States was estimated to be approximately 25%. It is important
to note that this percentage does not consider women with pelvic
pain due to high-tone pelvic floor dysfunction.
People with pelvic floor disorders benefit from an interdisciplinary
rehabilitation approach to improve function and reduce pain.
Physiatrists with experience in acute and chronic pain, neurologic
and musculoskeletal conditions, and neurogenic bowel/bladder
management are well suited to direct such a patient’s care.In
addition to diagnosing and managing the patient’s pelvic floor
disorder medically, the physiatrist plays a key role in providing
a detailed prescription for physical therapy.
Ergonomic modification for a person with a desk jobJoe Antony
It was estimated that about 40.7 % of the global population was surfing the computers in the year 2012 as compared to 2006 of only 26.2%. [1]
Marshall et al study reveal that on average, six out of 10 employees used a chair at work and the number was expected to grow.[2]
Many researchers report that working 5.41 hours sitting at desk and 7 hour sleeping at night had a great impact on the physical and mental health.[2]
Sitting on a chair is one of the most common positions adopted by humans.
children and adults spend approx. 55% of their working hours or 7.7 hours/day in sitting postures.[2]
The ergonomic fit workstations have become a standard practice in various developed countries
A special HKAFO, which uses a mechanical linkage to couple flexion of one hip with extension of the other, which enables a reciprocal step-over-step gait.
Also allow swing through and swing to gaits
Prevent knee buckling without actually including knee in orthosis
Sense of freedom and more control over external devices
Light weight- 300gms
Cosmetically acceptable
Prevents pressure sore
Easy maintenance
Total contact cast is rigid or semi-rigid molded cast which extends from the patient’s foot to just below the knee, maintaining contact with the entire plantar surface of the foot and lower leg and immobilizing surrounding joints and soft tissue while allowing the patient to remain ambulatory.
Considered as gold standard of offloading techniques
Started in early 1930s as a treatment modality for post hansens neuropathic ulcer
Effective , Rapid and ambulatory
BOTOX dosage in Lower Limb Spasticity.pptxJoe Antony
Botox injections are noted primarily for the ability to reduce the appearance of facial wrinkles. They're also used to treat conditions such as neck spasms (cervical dystonia), excessive sweating (hyperhidrosis), an overactive bladder and lazy eye. Botox injections may also help prevent chronic migraines
Synthetic Fiber Construction in lab .pptxPavel ( NSTU)
Synthetic fiber production is a fascinating and complex field that blends chemistry, engineering, and environmental science. By understanding these aspects, students can gain a comprehensive view of synthetic fiber production, its impact on society and the environment, and the potential for future innovations. Synthetic fibers play a crucial role in modern society, impacting various aspects of daily life, industry, and the environment. ynthetic fibers are integral to modern life, offering a range of benefits from cost-effectiveness and versatility to innovative applications and performance characteristics. While they pose environmental challenges, ongoing research and development aim to create more sustainable and eco-friendly alternatives. Understanding the importance of synthetic fibers helps in appreciating their role in the economy, industry, and daily life, while also emphasizing the need for sustainable practices and innovation.
Honest Reviews of Tim Han LMA Course Program.pptxtimhan337
Personal development courses are widely available today, with each one promising life-changing outcomes. Tim Han’s Life Mastery Achievers (LMA) Course has drawn a lot of interest. In addition to offering my frank assessment of Success Insider’s LMA Course, this piece examines the course’s effects via a variety of Tim Han LMA course reviews and Success Insider comments.
The Roman Empire A Historical Colossus.pdfkaushalkr1407
The Roman Empire, a vast and enduring power, stands as one of history's most remarkable civilizations, leaving an indelible imprint on the world. It emerged from the Roman Republic, transitioning into an imperial powerhouse under the leadership of Augustus Caesar in 27 BCE. This transformation marked the beginning of an era defined by unprecedented territorial expansion, architectural marvels, and profound cultural influence.
The empire's roots lie in the city of Rome, founded, according to legend, by Romulus in 753 BCE. Over centuries, Rome evolved from a small settlement to a formidable republic, characterized by a complex political system with elected officials and checks on power. However, internal strife, class conflicts, and military ambitions paved the way for the end of the Republic. Julius Caesar’s dictatorship and subsequent assassination in 44 BCE created a power vacuum, leading to a civil war. Octavian, later Augustus, emerged victorious, heralding the Roman Empire’s birth.
Under Augustus, the empire experienced the Pax Romana, a 200-year period of relative peace and stability. Augustus reformed the military, established efficient administrative systems, and initiated grand construction projects. The empire's borders expanded, encompassing territories from Britain to Egypt and from Spain to the Euphrates. Roman legions, renowned for their discipline and engineering prowess, secured and maintained these vast territories, building roads, fortifications, and cities that facilitated control and integration.
The Roman Empire’s society was hierarchical, with a rigid class system. At the top were the patricians, wealthy elites who held significant political power. Below them were the plebeians, free citizens with limited political influence, and the vast numbers of slaves who formed the backbone of the economy. The family unit was central, governed by the paterfamilias, the male head who held absolute authority.
Culturally, the Romans were eclectic, absorbing and adapting elements from the civilizations they encountered, particularly the Greeks. Roman art, literature, and philosophy reflected this synthesis, creating a rich cultural tapestry. Latin, the Roman language, became the lingua franca of the Western world, influencing numerous modern languages.
Roman architecture and engineering achievements were monumental. They perfected the arch, vault, and dome, constructing enduring structures like the Colosseum, Pantheon, and aqueducts. These engineering marvels not only showcased Roman ingenuity but also served practical purposes, from public entertainment to water supply.
Model Attribute Check Company Auto PropertyCeline George
In Odoo, the multi-company feature allows you to manage multiple companies within a single Odoo database instance. Each company can have its own configurations while still sharing common resources such as products, customers, and suppliers.
The French Revolution, which began in 1789, was a period of radical social and political upheaval in France. It marked the decline of absolute monarchies, the rise of secular and democratic republics, and the eventual rise of Napoleon Bonaparte. This revolutionary period is crucial in understanding the transition from feudalism to modernity in Europe.
For more information, visit-www.vavaclasses.com
Unit 8 - Information and Communication Technology (Paper I).pdfThiyagu K
This slides describes the basic concepts of ICT, basics of Email, Emerging Technology and Digital Initiatives in Education. This presentations aligns with the UGC Paper I syllabus.
Read| The latest issue of The Challenger is here! We are thrilled to announce that our school paper has qualified for the NATIONAL SCHOOLS PRESS CONFERENCE (NSPC) 2024. Thank you for your unwavering support and trust. Dive into the stories that made us stand out!
Introduction to AI for Nonprofits with Tapp NetworkTechSoup
Dive into the world of AI! Experts Jon Hill and Tareq Monaur will guide you through AI's role in enhancing nonprofit websites and basic marketing strategies, making it easy to understand and apply.
How to Make a Field invisible in Odoo 17Celine George
It is possible to hide or invisible some fields in odoo. Commonly using “invisible” attribute in the field definition to invisible the fields. This slide will show how to make a field invisible in odoo 17.
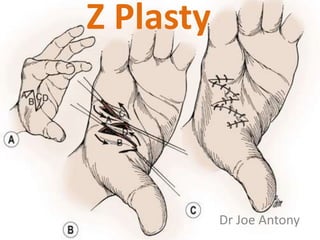
2. • The Z-plasty is a procedure which involves the
transposition of two inter-digitating triangular
flaps
• First performed by Horner in 1837 and
Denonvilliers in 1854.
– They used to correct cicatricial ectropion
• The first published mathematical analysis
came from Limberg in 1929.
3. • Limberg used pythogorian theory to derive
length achieved by each angles
4. Principles
• 1. There is a gain in length along the direction
of the common limb of the Z.
• 2. The direction of the common limb of the Z
is changed.
6. • the length of the contractural diagonal after
transposition equals that of the transverse
diagonal before transposition.
– unless there is transverse skin slack available,
equal in quantity to the length difference between
the axes of the Z, the method will not work.
11. Blood supply of flaps
• Provision of maximum vascularity
– designing the flaps broad at the tip
– by cutting the flaps as thick as possible
– avoiding scarring across the base
• Avoidance of undue tension
– Tip necrosis in single large Z plasty.
13. Simple Z plasty
• stereometric Z-plasty
• two flaps of equal angle and length
• Raised at 60° as this angle offers the best
balance between elongation in the axis of the
scar and the creation of tension forces pulling
perpendicular to the scar.
14. Planimetric Z plasty
• By minimizing the amount of rotation and
excising redundant tissue, this flap design
avoids the contours and depressions
15. • May theoretically be designed with lateral
limb angles ranging from 60° to 90°, though
most often they are planned at 75° angles
• Planimetric Z-plasty is ideal for scar releases
on flat surfaces where lengthening is the
primary objective and contour deformities
would be suboptimal.
16. Skew Z plasties
• Skew Z-plasties have lateral limbs departing at
different angles from one another.
• This flap has been suggested when anatomic
landmarks mandate asymmetric movement of
one flap.
17. • Narrow flap form dog ear while suturing
• Wide flap has more tension over the base ,
causing restricted blood supply to the flap tip
18. Contracture release
• Adequate amount of free skin must be
available transversly
• Burns contracture- Usually with surrounding
skin scarring
19.
20.
21. Planning of Z plasty
• Draw equilateral triangle on both sides
• 1. The flap with the better blood supply is
preferable. In particular a potential flap with
scarring across the base should be avoided.
• 2. One flap may result in a scar which will fall
into a better line cosmetically.
• 3. The lie of the flaps and the surrounding
skin may permit one set of flaps to transpose
more readily into their new position.