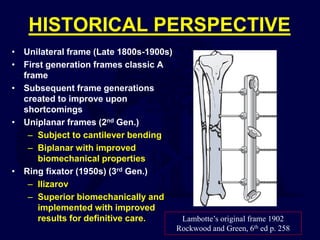
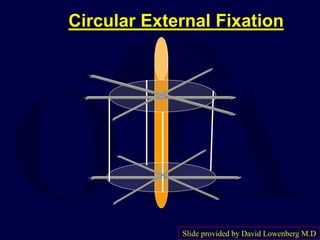
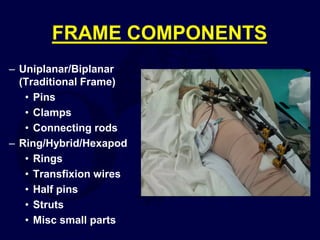
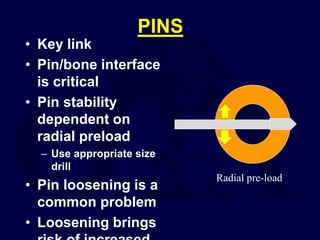
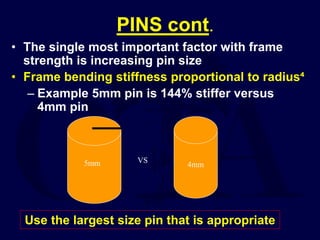
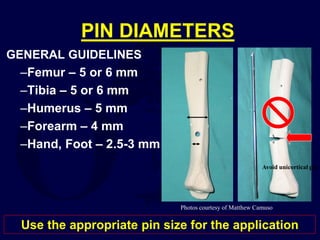
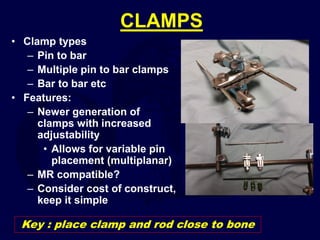
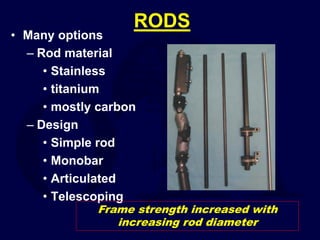
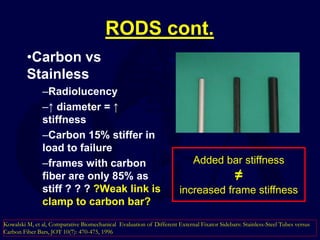
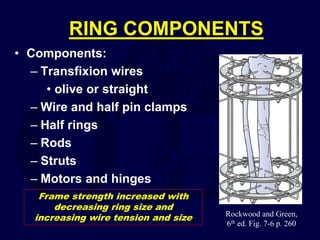
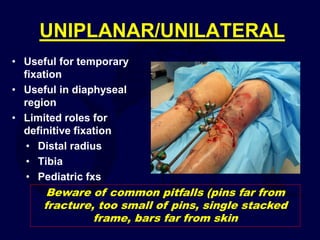
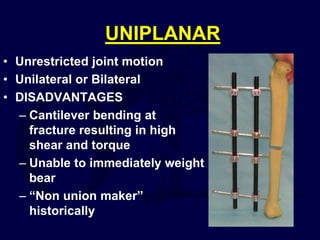
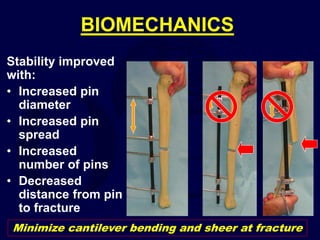
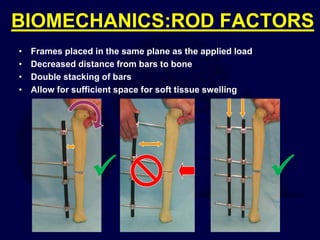
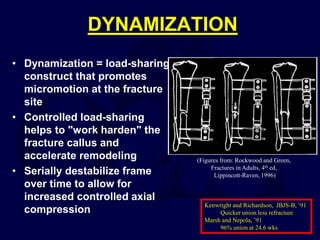
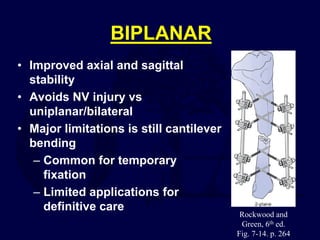
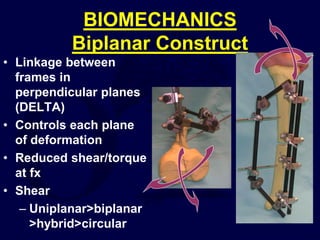
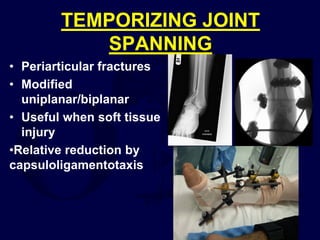
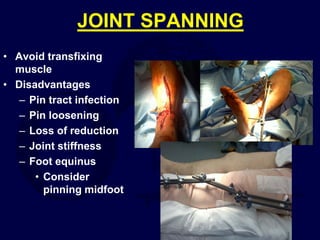
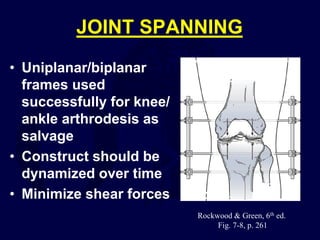
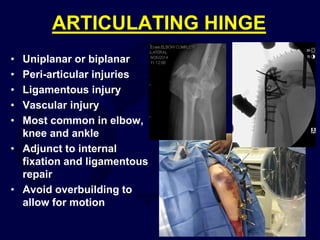
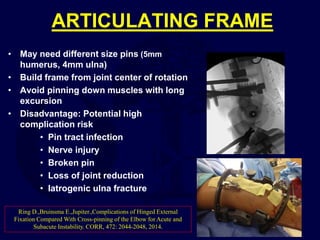
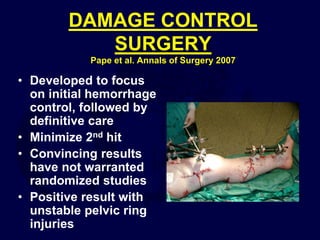
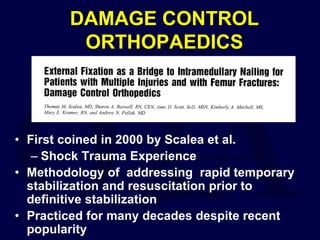
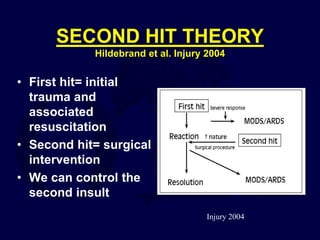
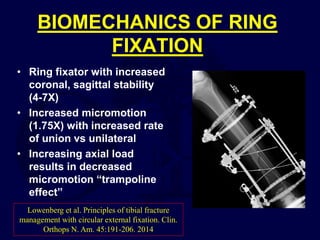
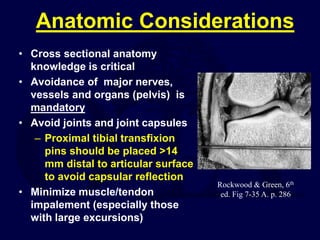
This document provides an overview of the principles of external fixation. It discusses the historical progression of external fixator designs from 1st generation rigid frames to modern circular and hexapod frames. Key components of external fixation like pins, clamps, and rods are described. The document emphasizes improving frame stability through increasing pin size and decreasing the distance between pins and fractures. It covers applications of uniplanar, biplanar, circular, and articulating frames and discusses the concept of damage control surgery using temporary external fixation.