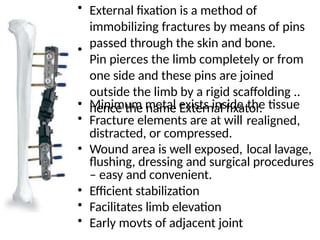
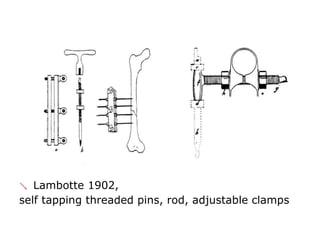
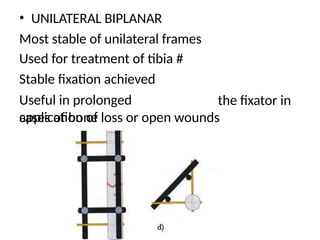
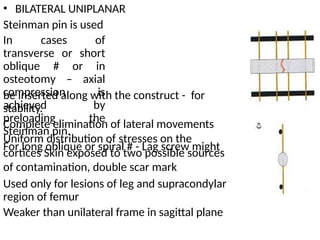
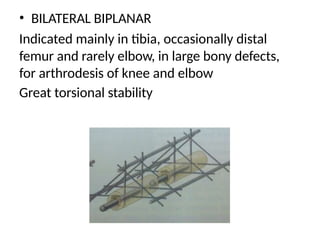
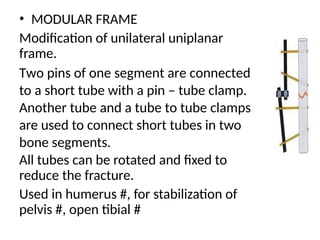
External fixators are devices used to immobilize fractures by securing pins externally, allowing for better wound access and tissue management. The method has evolved from ancient techniques to modern application with advances like the Ilizarov apparatus for limb lengthening and deformity correction. There are two main types of fixators: pin fixators and ring fixators, each with distinct advantages and drawbacks in terms of stability and soft tissue access.