Downloaded 76 times

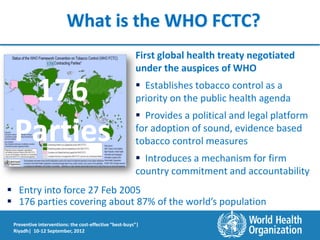
![Exposure to second-hand smoke also kills
Distribution of
One third of adults are regularly total deaths
attributable to
exposed to second-hand tobacco SHS, 2004
smoke.
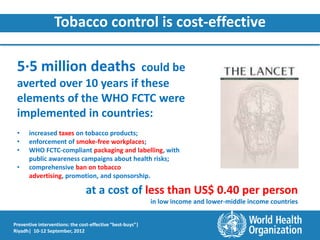
About 600 000 people die each year
as a result of exposure to second-
hand smoke.
• 430 000 are adults, of whom 64% are women
• 28% of the second-hand smoke deaths are
among children
Source: Global estimate of the burden of disease Mattias Oberg … [et al], WHO 2010,
http://www.who.int/tobacco/publications/second_hand/global_estimate_burden_disease/en/index.html
.
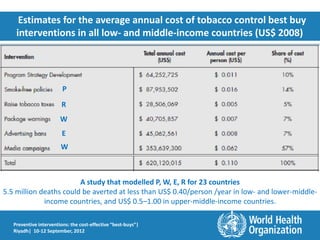
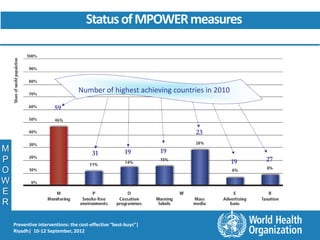
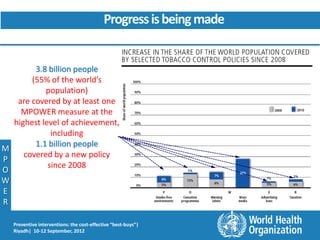
Preventive interventions: the cost-effective “best-buys”|
Riyadh| 10-12 September, 2012](https://image.slidesharecdn.com/tcdraft7sept2012riyadh-rev-120912015501-phpapp02/85/Preventive-Interventions-The-cost-effective-Best-Buys-8-320.jpg)











!["We have evidence, and we have instruments"
Dr Margaret Chan, Director-General of the World Health Organization
Keynote address at the 15th World Conference on Tobacco or Health, Singapore, 20 March 2012
"As a tool for fighting back, we "And we have an enemy, […] the
have the WHO FCTC. We have a tobacco industry, has changed its face
practical, cost-effective way to and its tactics. Tactics aimed at
scale up implementation of undermining anti-tobacco
provisions in the treaty on the campaigns, and subverting the WHO
ground. […] the best-buy and FCTC, are no longer covert or cloaked
good-buy measures for by an image of corporate social
reducing tobacco use set out in responsibility. They are out in the open
the MPOWER package." and they are extremely aggressive"
"[…] full implementation of the "I called on heads of state and
WHO FCTC would deliver the government to stand rock-hard
single biggest preventive blow to against the despicable efforts of
heart disease, cancer, diabetes, the tobacco industry to subvert
and respiratory disease." this treaty."
Preventive interventions: the cost-effective “best-buys”|
Riyadh| 10-12 September, 2012](https://image.slidesharecdn.com/tcdraft7sept2012riyadh-rev-120912015501-phpapp02/85/Preventive-Interventions-The-cost-effective-Best-Buys-38-320.jpg)

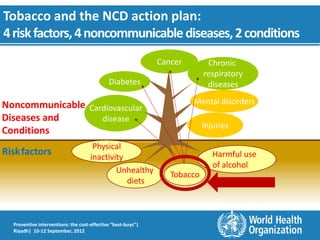
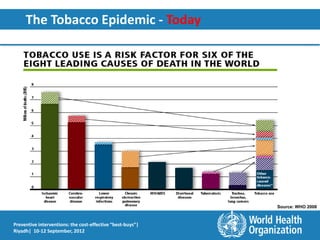
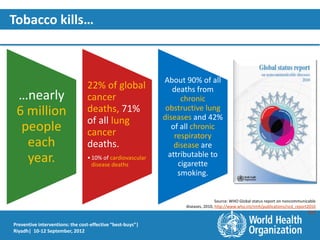
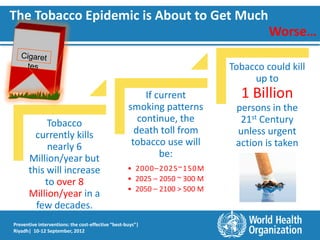
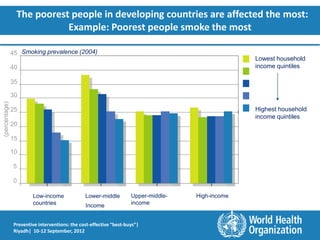
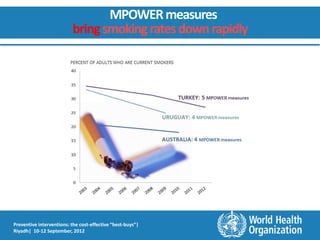
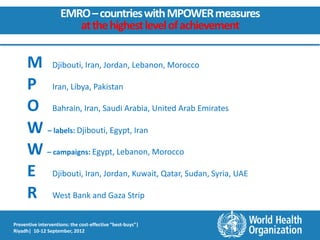
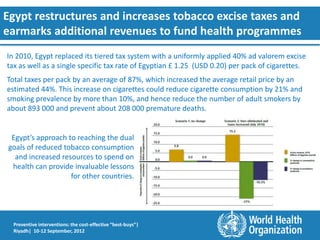
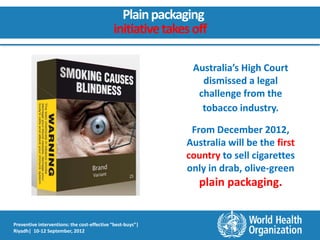
This document discusses tobacco control interventions as cost-effective "best buys" for preventing noncommunicable diseases. It outlines the tobacco epidemic and impact on health and economies. The WHO Framework Convention on Tobacco Control and MPOWER strategies are presented as evidence-based mechanisms for implementing demand reduction measures like tax increases and protection from smoke, as well as supply measures. Case studies show progress in implementing strong warning labels, advertising bans, and tax increases in countries like Iran, Jordan, and Egypt. Tobacco control is estimated to avert over 5 million deaths at relatively low cost.



















































![Tob control. 2010_dec_19(6)_457-62[1]](https://cdn.slidesharecdn.com/ss_thumbnails/tobcontrol-2010dec196457-621-110509233432-phpapp02-thumbnail.jpg?width=640&height=640&fit=bounds)







































