Download to read offline
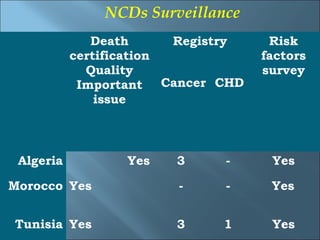




This document summarizes an experience in managing non-communicable diseases (NCDs) in North Africa. It examines preparedness in Algeria, Morocco, and Tunisia to address rising NCD rates due to similar cultures, lifestyles, and health systems following French colonization. NCDs cause over half of deaths in the region. While national NCD programs were implemented in the 1990s, 2008-2013 action plans were not fully realized. Surveillance and risk factor data exist but health systems remain fragmented. Multisector collaboration and sustainable financing models are needed to curb NCDs in Northern Africa through strengthened regional partnerships.


































































![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)















