Downloaded 456 times

![Cost effective interventions to address
NCDs
Population-based
interventions
addressing
NCD
risk factors
Tobacco use - Excise tax increases
- Smoke-free indoor workplaces and public places
- Health information and warnings about tobacco
- Bans on advertising and promotion
Harmful use
of alcohol
- Excise tax increases on alcoholic beverages
- Comprehensive restrictions and bans on alcohol marketing
- Restrictions on the availability of retailed alcohol
Unhealthy
diet and
physical
inactivity
- Salt reduction through mass media campaigns and reduced salt
content in processed foods
- Replacement of trans-fats with polyunsaturated fats
- Public awareness programme about diet and physical activity
Individual-based
interventions
addressing
NCDs in
primary care
Cancer - Prevention of liver cancer through hepatitis B immunization
- Prevention of cervical cancer through screening (visual
inspection with acetic acid [VIA]) and treatment of pre-cancerous
lesions
CVD and
diabetes
- Multi-drug therapy (including glycaemic control for diabetes
mellitus) for individuals who have had a heart attack or stroke,
and to persons at high risk (> 30%) of a cardiovascular event
within 10 years
- Providing aspirin to people having an acute heart attack
19](https://image.slidesharecdn.com/overviewofncdlead-ncd-malworkshopdec2014-141201095635-conversion-gate02/75/Overview-of-Non-Communicable-Diseases-19-2048.jpg)


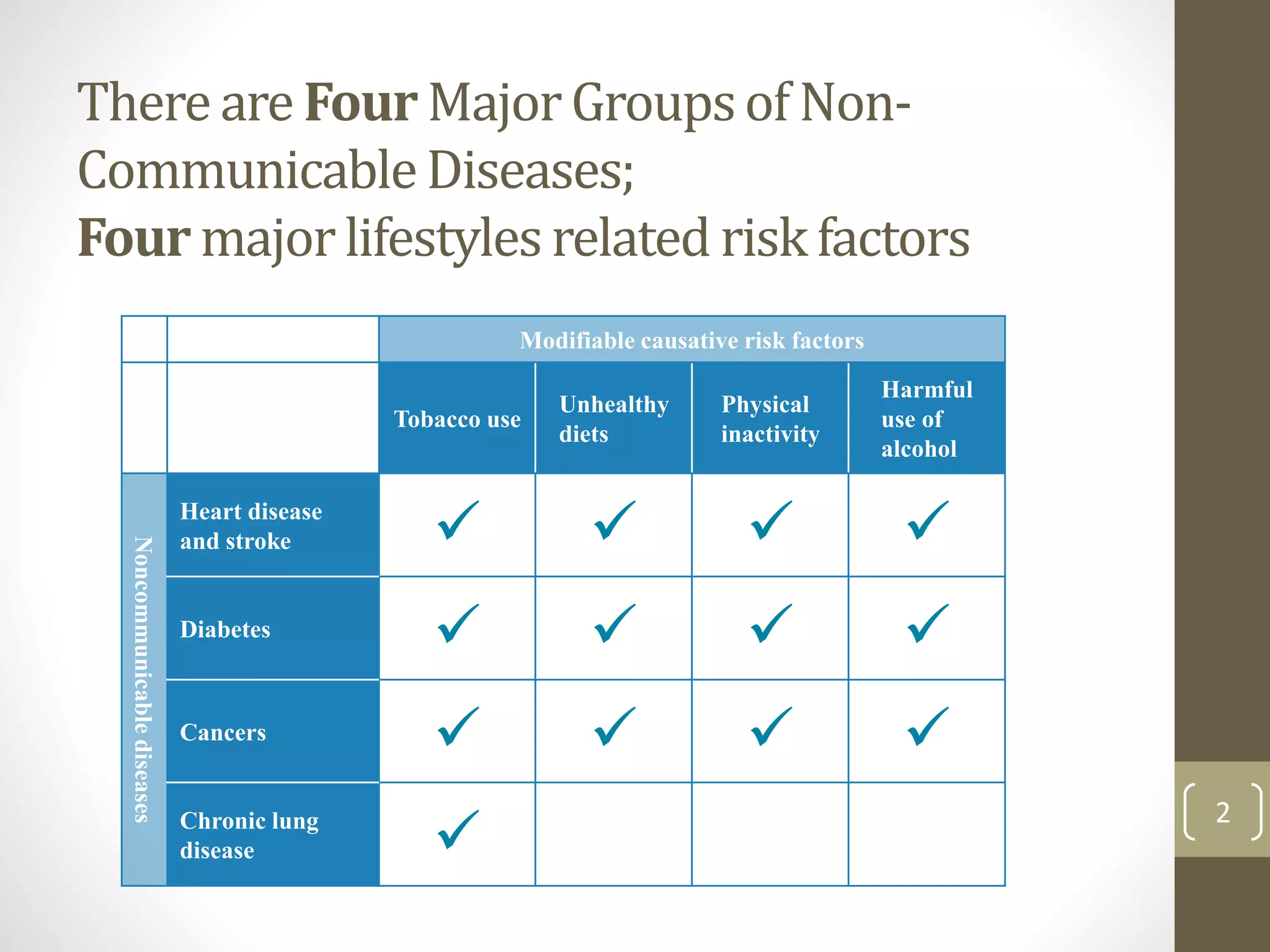
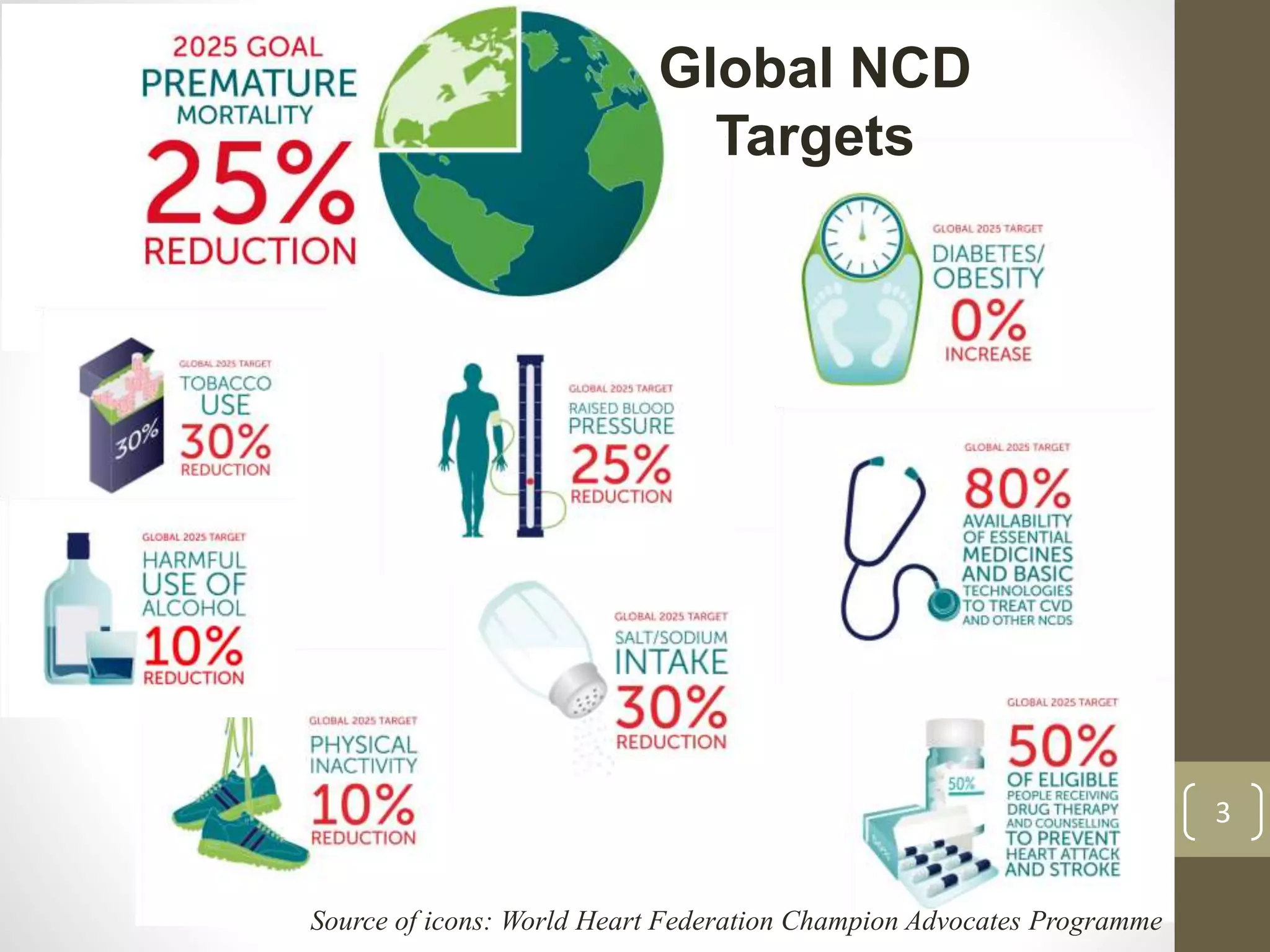
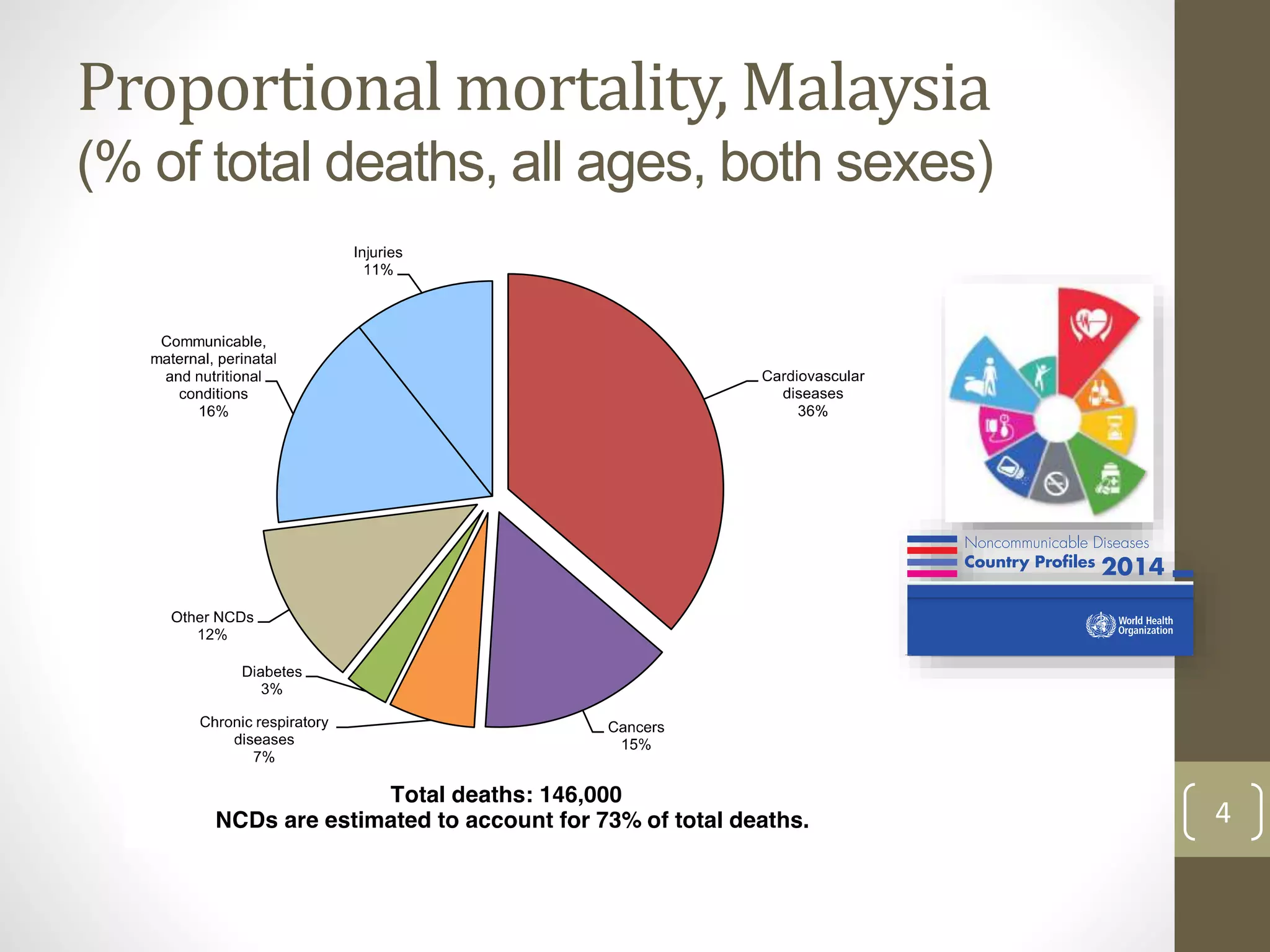
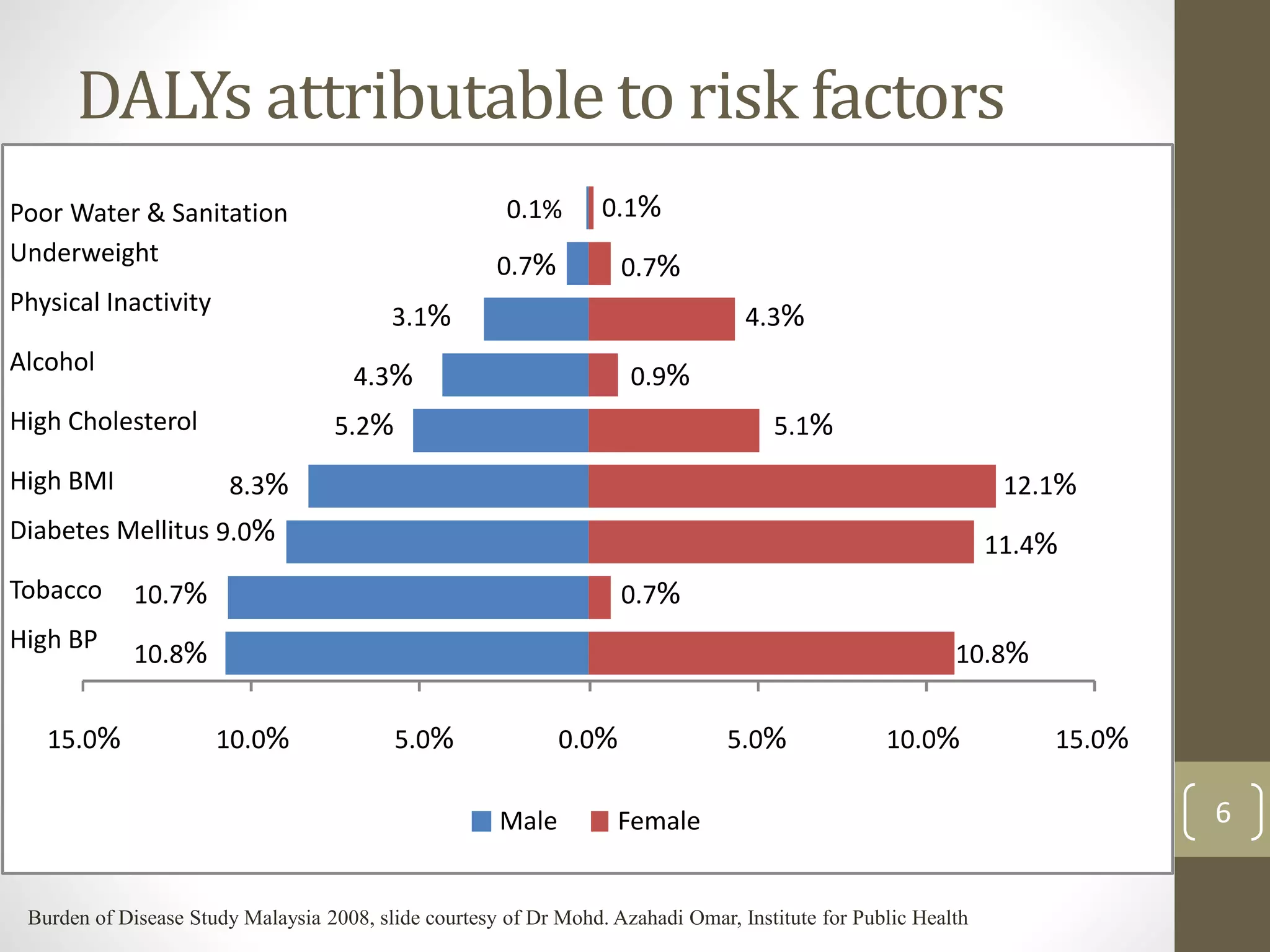
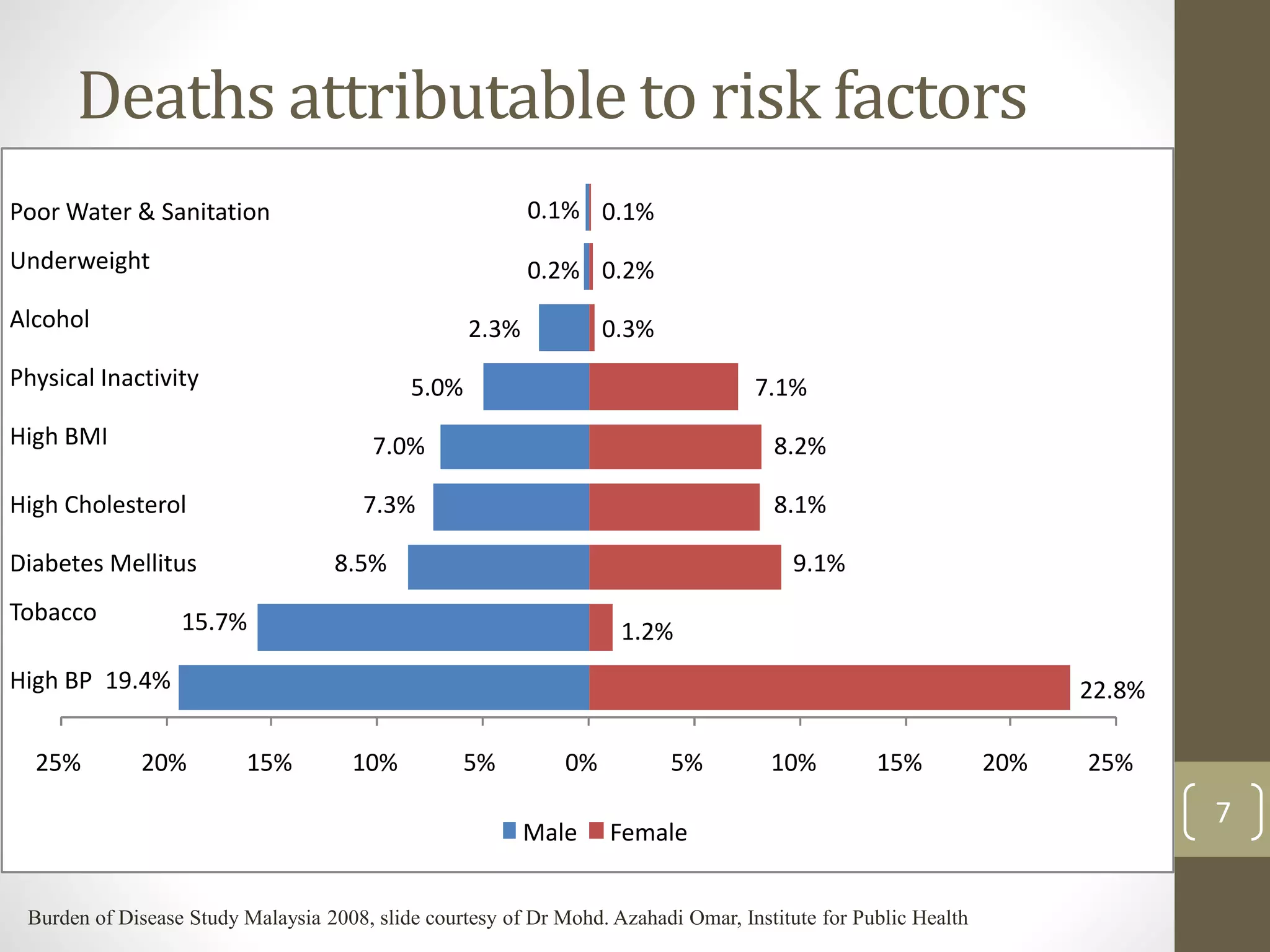
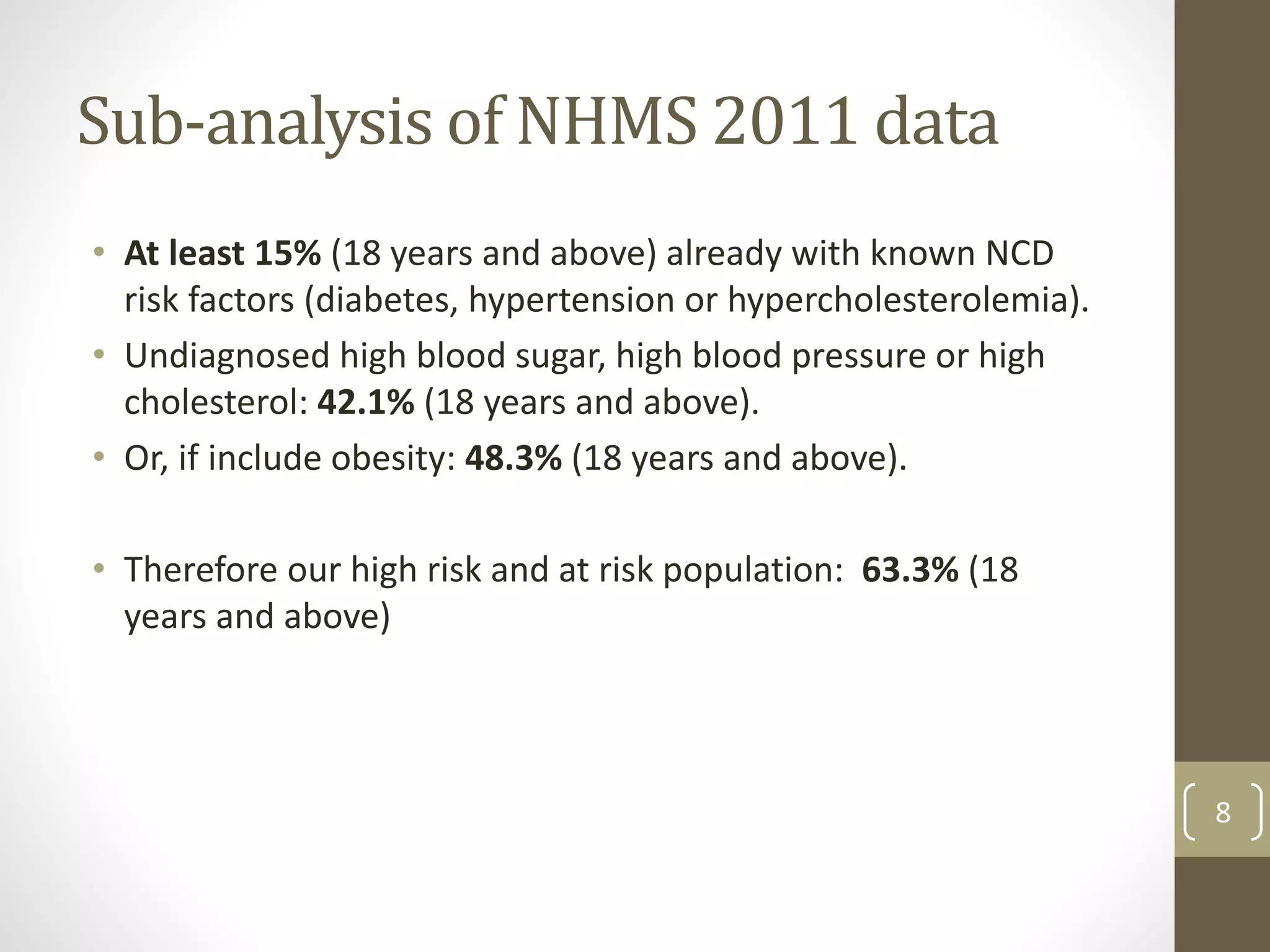
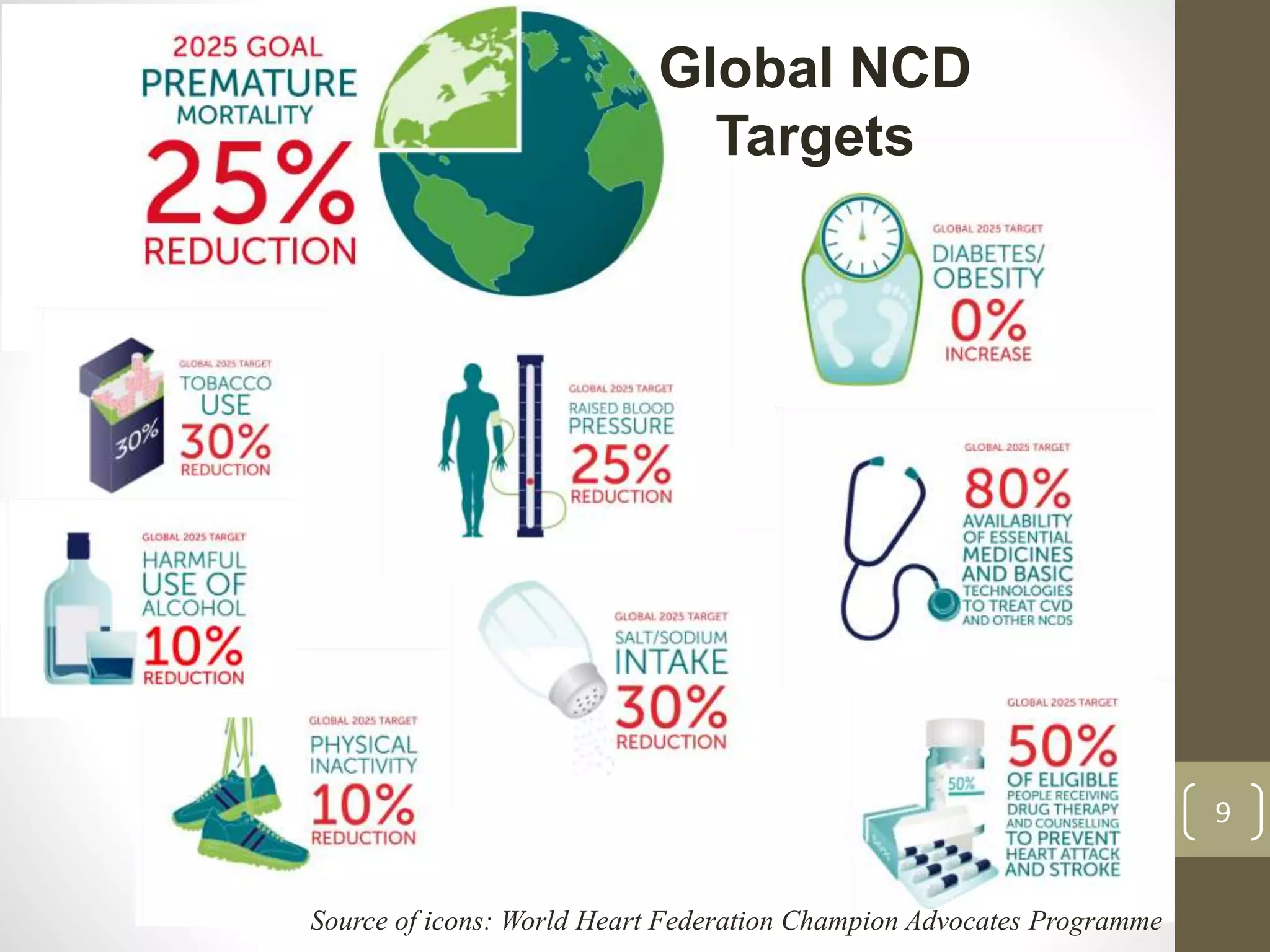
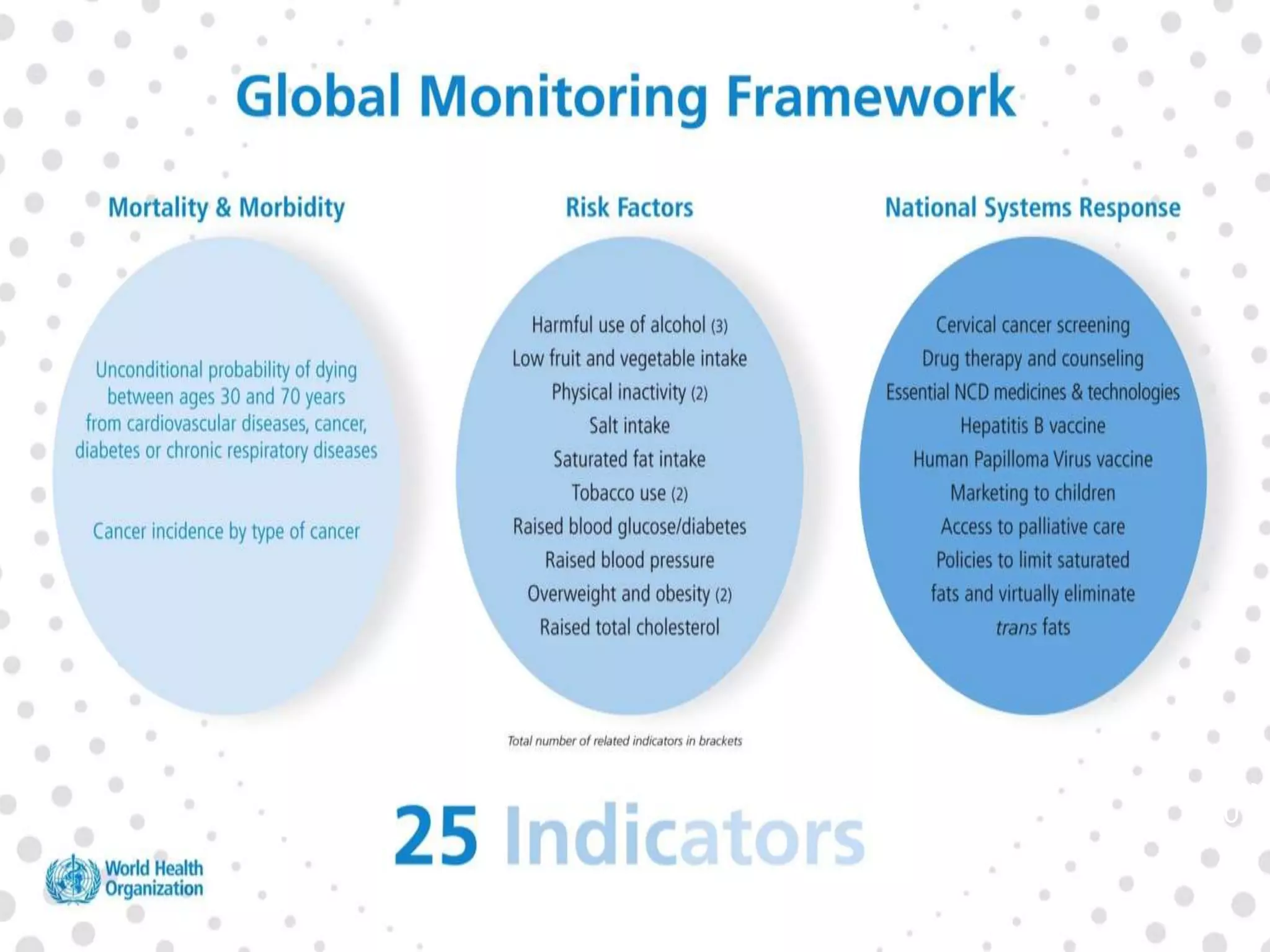
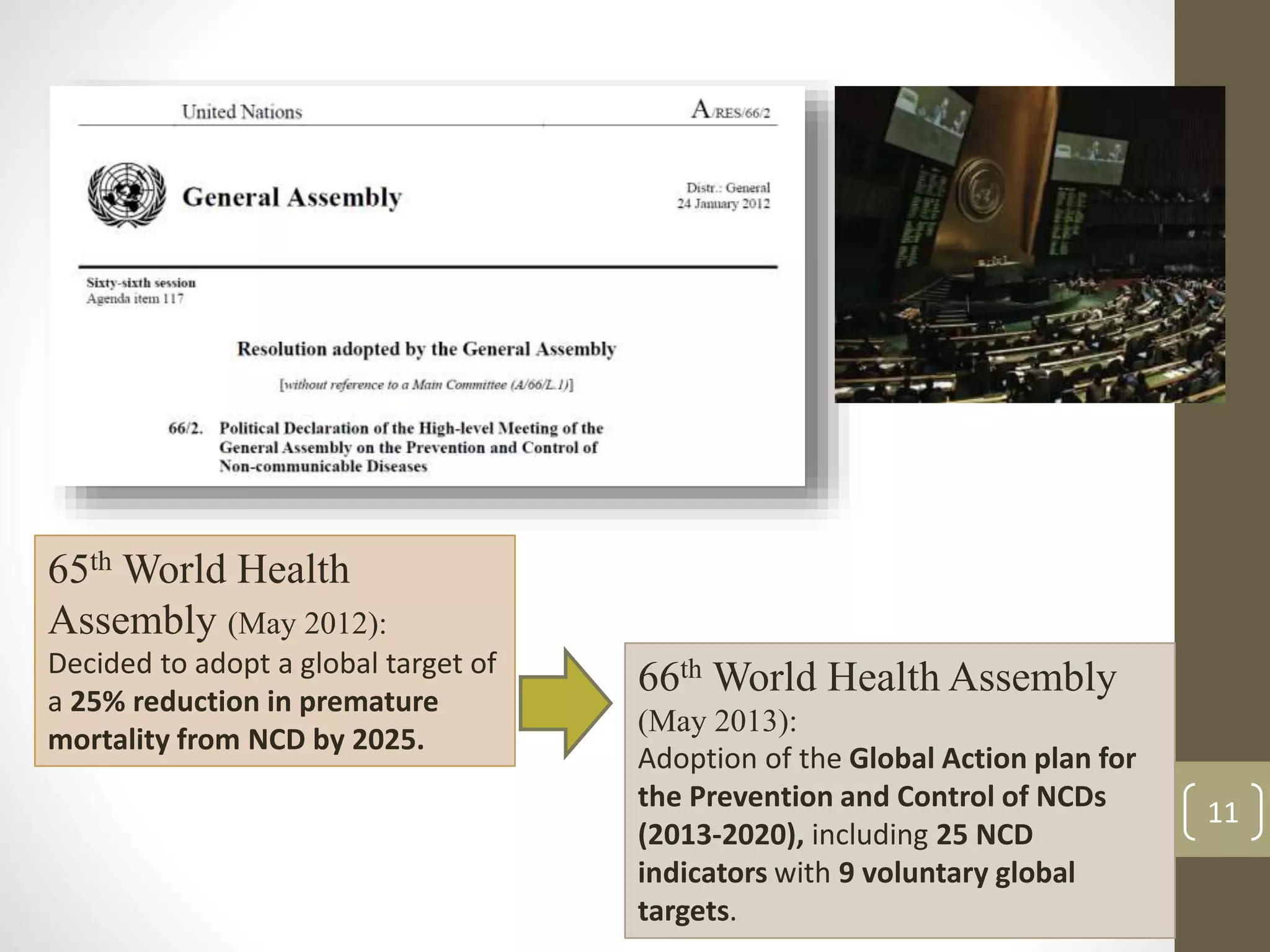
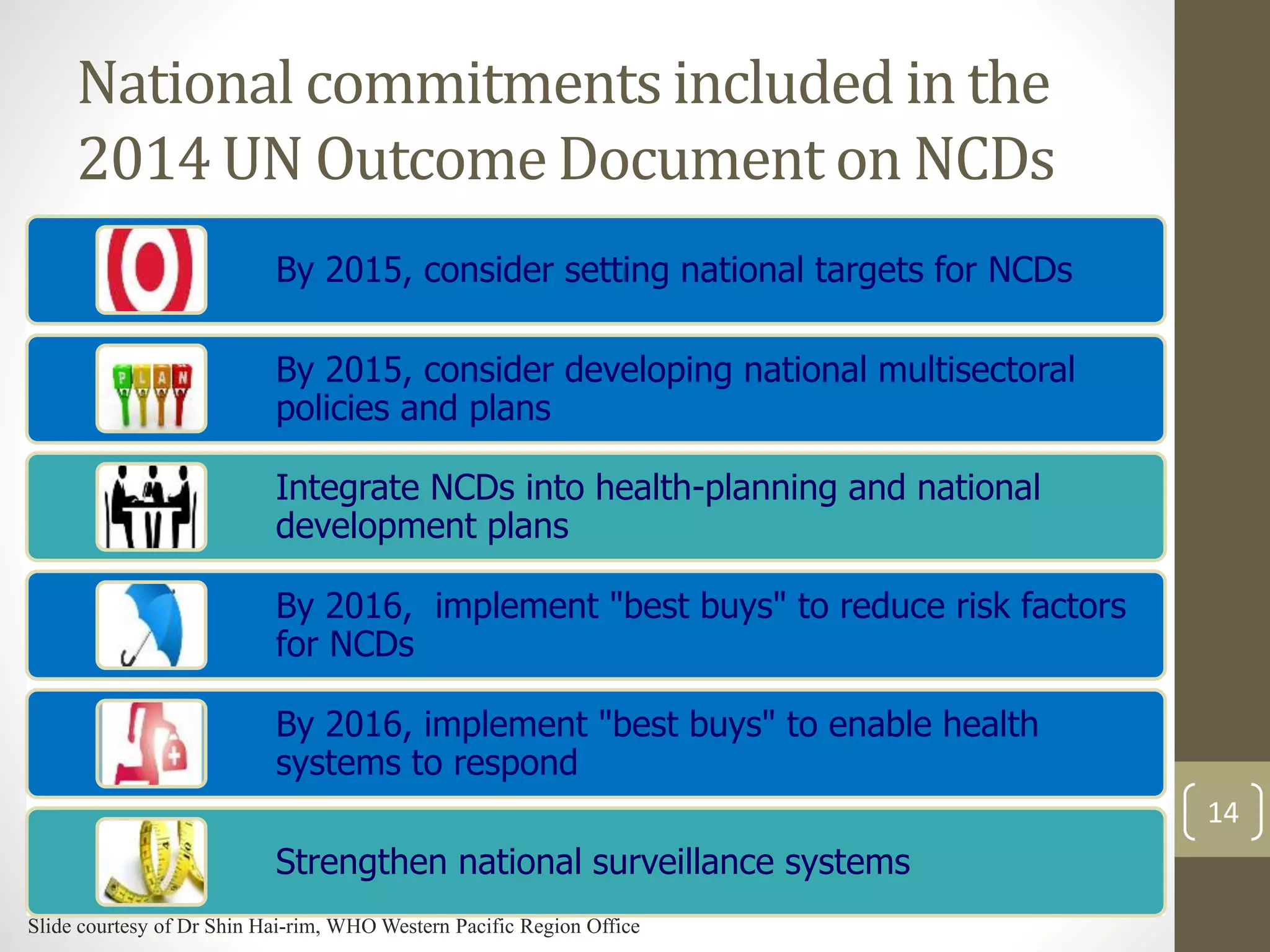
The document provides an overview of non-communicable diseases (NCDs) in Malaysia, outlining major conditions and lifestyle-related risk factors such as tobacco use and unhealthy diets. It emphasizes the urgent need for a multi-sectoral approach to effectively prevent and control NCDs, which are increasing in prevalence and significantly affect both health and economic development. The document also highlights commitments made at global health assemblies to reduce premature mortality from NCDs by 25% by 2025.











































































![Management of diabetes in malaysia, istanbul 2013[final]](https://cdn.slidesharecdn.com/ss_thumbnails/managementofdiabetesinmalaysiaistanbul2013final-131123092516-phpapp02-thumbnail.jpg?width=640&height=640&fit=bounds)





















