Downloaded 113 times










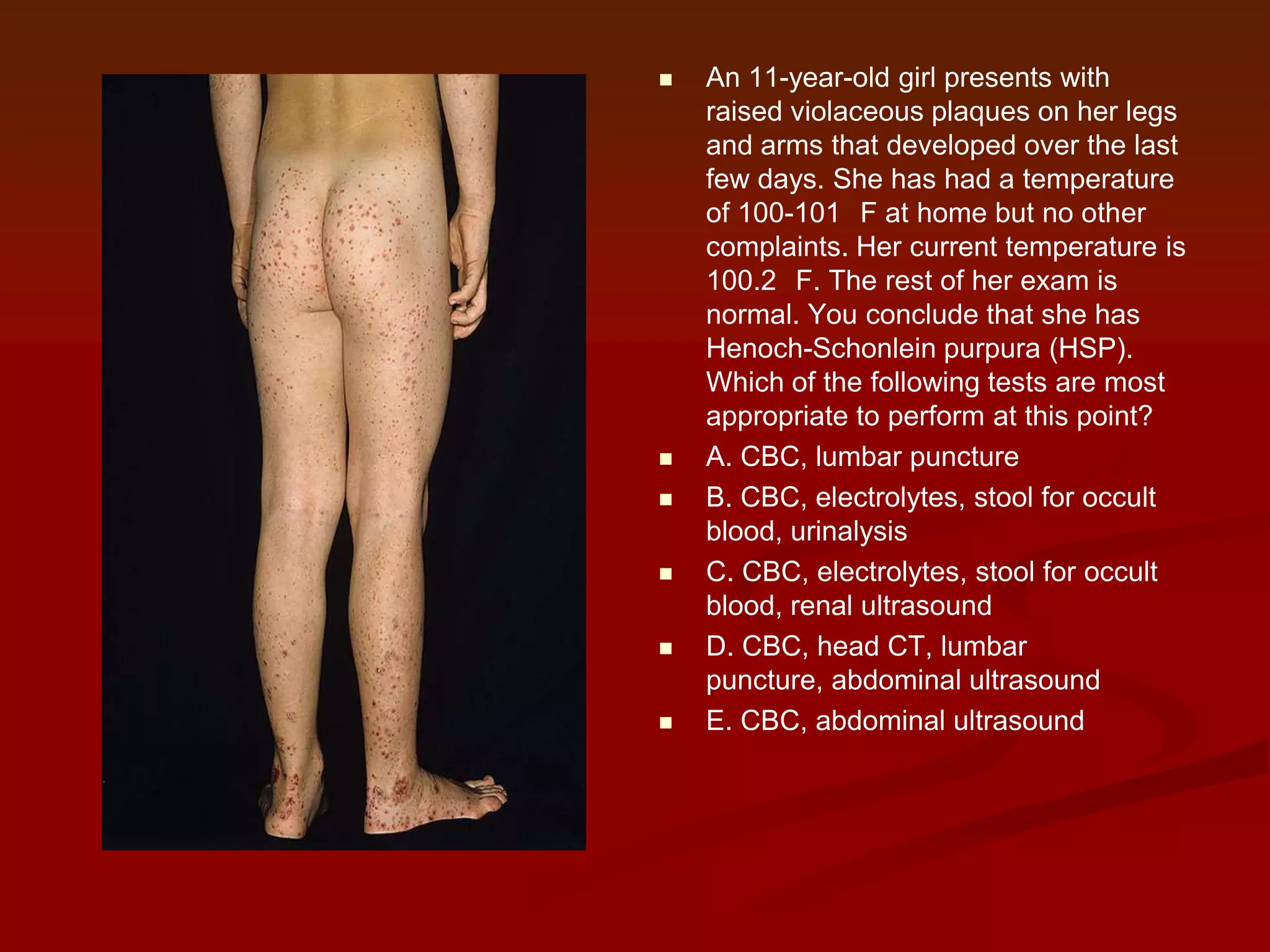


A pediatric patient presented with fever and a rash, which can indicate various illnesses ranging from minor to life-threatening. The differential diagnosis for febrile patients with a rash is extensive, including viral, bacterial, and other infectious etiologies. Proper evaluation and management of these patients is important as the severity of illness can vary greatly.





















![Approach to a_child_with_rash[1]](https://cdn.slidesharecdn.com/ss_thumbnails/approachtoachildwithrash1-180504150522-thumbnail.jpg?width=640&height=640&fit=bounds)









































































![Apporach to lung biopsy [Auto-saved].pptx latest](https://cdn.slidesharecdn.com/ss_thumbnails/apporachtolungbiopsyauto-saved-251211225655-93258539-thumbnail.jpg?width=640&height=640&fit=bounds)






