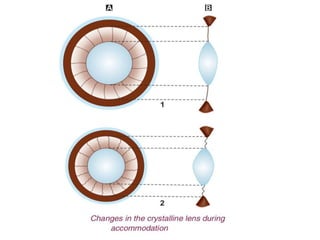
This document discusses presbyopia, an age-related condition characterized by a loss of ability to focus on near objects. It defines key terms like accommodation, near and far points. Presbyopia is caused by hardening of the lens and decreased elasticity of lens fibers with age. Symptoms include difficulty with near vision. Presbyopia treatment involves prescribing convex lenses matched to the patient's age to allow clear near vision. Multifocal lenses can provide both distance and near correction.