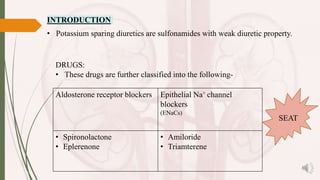
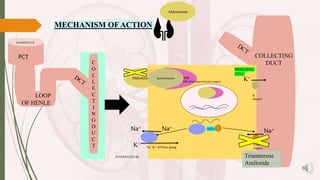
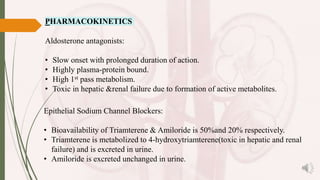
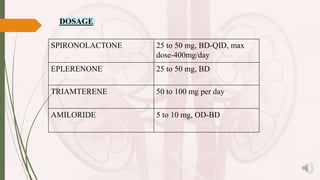
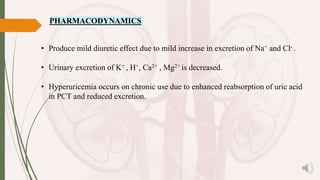
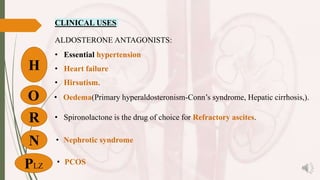
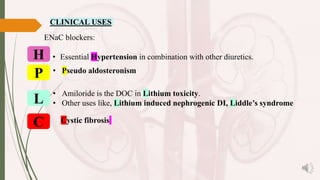
Potassium-sparing diuretics are categorized into aldosterone receptor blockers and epithelial Na+ channel blockers, including drugs like spironolactone, eplerenone, amiloride, and triamterene. They are used for various conditions such as hypertension, heart failure, and hirsutism, but can cause side effects like hyperkalemia and metabolic acidosis. Precautions include avoiding use in patients with renal or hepatic failure, and caution with other medications like β-blockers and ACE inhibitors.






















































![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)











![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)

