Downloaded 289 times





![Data collected
•
•
•
•
•
•
AGE
Pre-op functional status
ASA score
BMI
OSA
Congestive heart failure hx [use NYHA if known or mild,
moderate, severe]
• Cigarette use
• Asthma/COPD
• Diabetes [IDDM/NIDDM]](https://image.slidesharecdn.com/postoperativepulmonarycomplications-131029172914-phpapp02/75/Postoperative-pulmonary-complications-9-2048.jpg)






























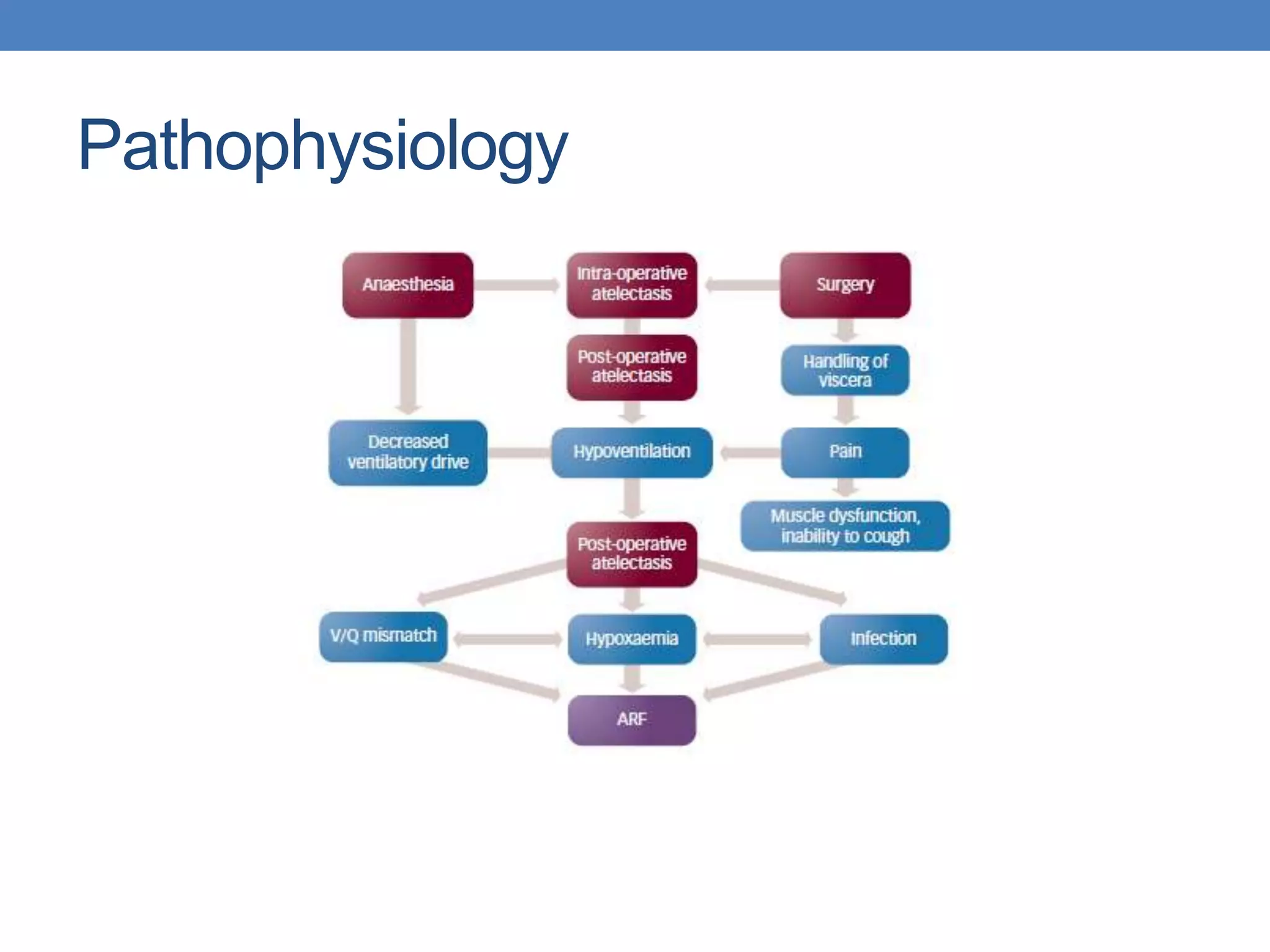
1. Post-operative pulmonary complications (PPCs) such as pneumonia, atelectasis, and acute lung injury are common after surgery, increasing mortality, length of hospital stay, and costs. 2. An audit was conducted of 102 patients undergoing major surgery to identify risk factors for PPCs and the rate of post-operative pneumonia. The overall PPC rate was 20.5% and the pneumonia rate was 14.7%. 3. High risk groups identified included those with ASA score of 3 or higher, pre-existing pulmonary disease, diabetes, smoking history, and surgeries over 180 minutes.


































































![PR CAMPAIGN 2011 [GERMANY]](https://cdn.slidesharecdn.com/ss_thumbnails/pipcarticleforanaeenglishfinal-130220045138-phpapp02-thumbnail.jpg?width=640&height=640&fit=bounds)





























