This document summarizes several types of maxillary nerve blocks:
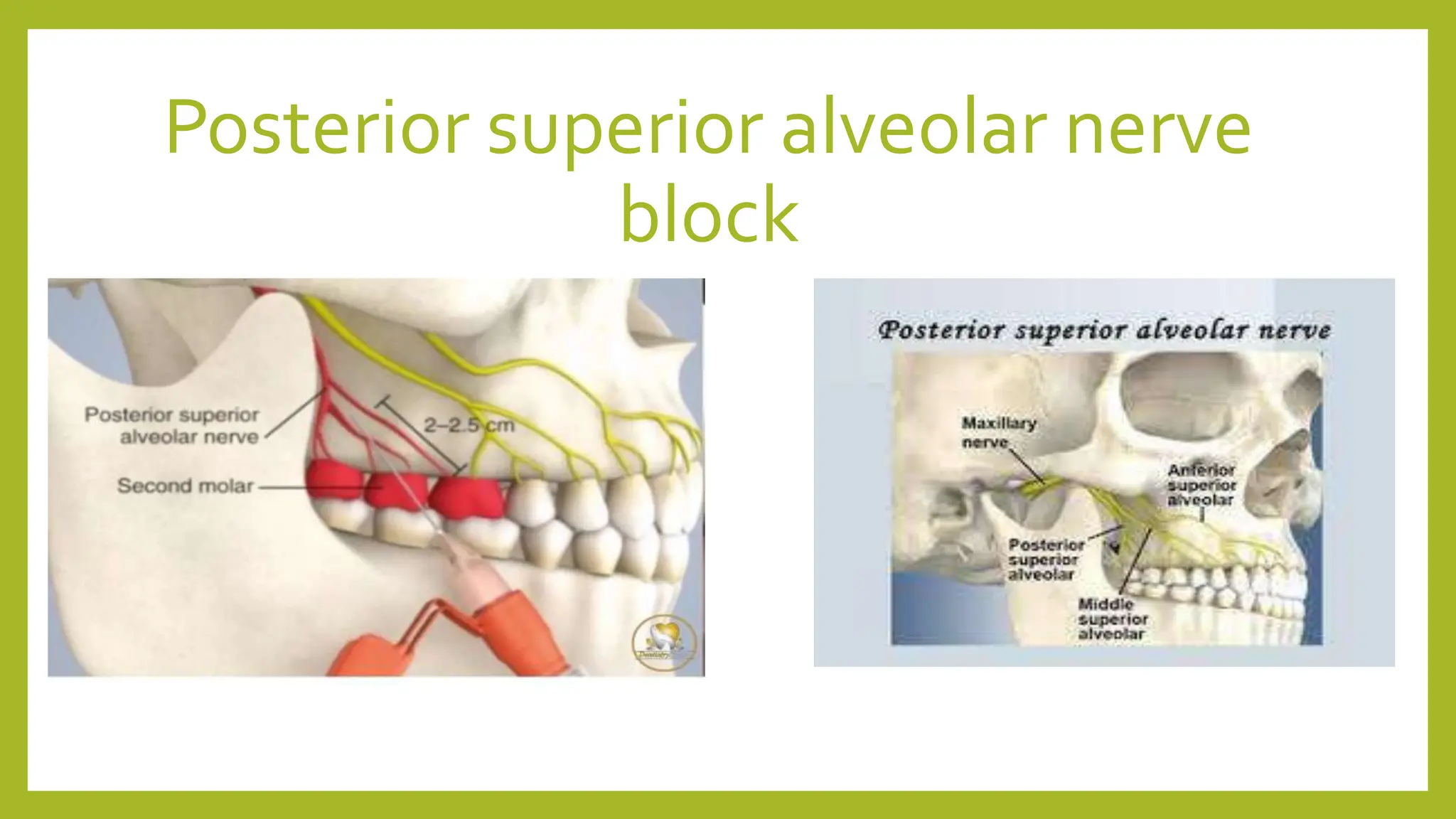
- Posterior superior alveolar nerve block anesthetizes the maxillary molars and surrounding structures. The needle is inserted behind the zygomatic process.
- Nasopalatine nerve block anesthetizes the anterior hard palate. The needle is inserted into the incisive papilla after a preparatory injection between the central incisors.
- Anterior palatine nerve block anesthetizes the posterior hard palate. The needle is slowly inserted until contacting the palatal bone opposite the maxillary molars.












































































![Local Anesthesia in childs [Autosaved].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/localanesthesiainchildsautosaved-240712192726-fceb4391-thumbnail.jpg?width=640&height=640&fit=bounds)
























