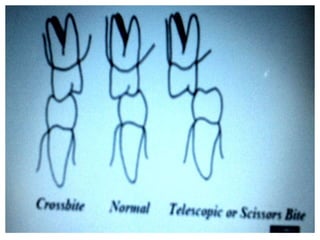
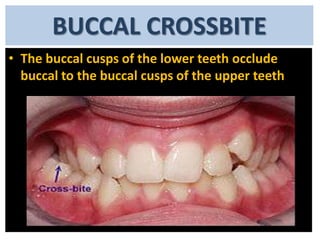
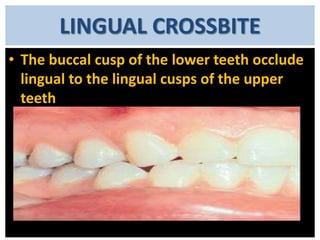
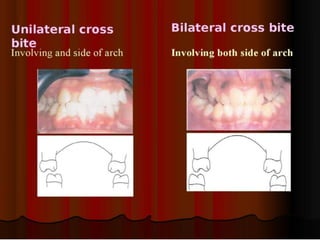
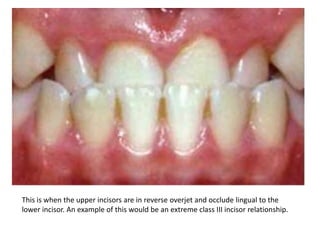
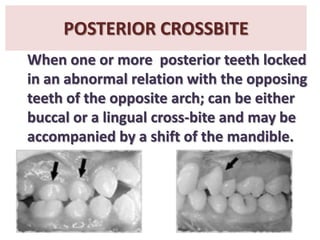
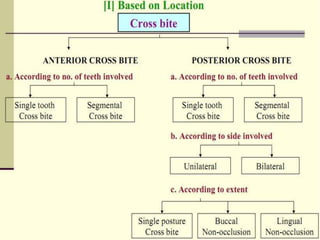
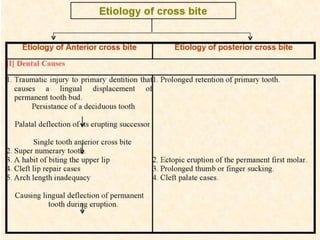
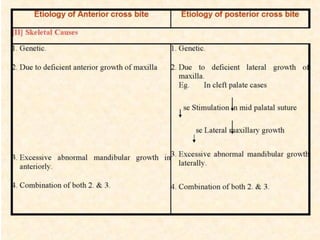
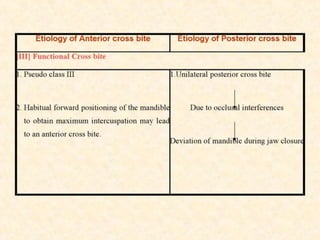
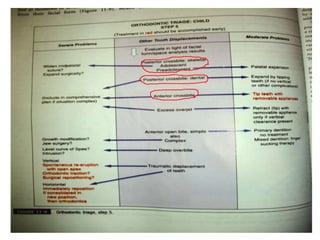
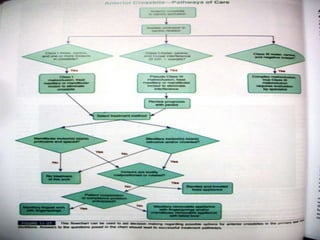
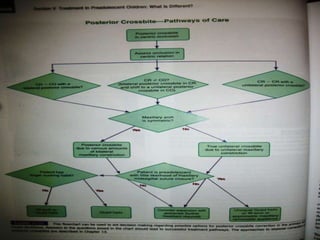
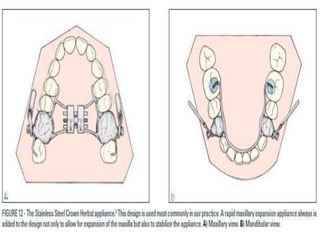
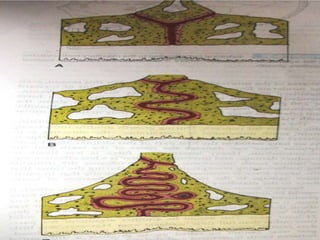
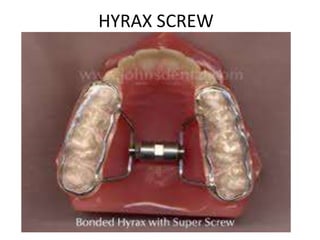
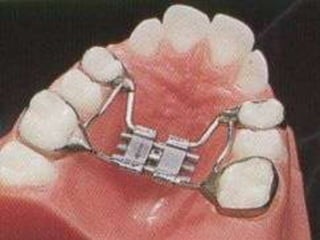
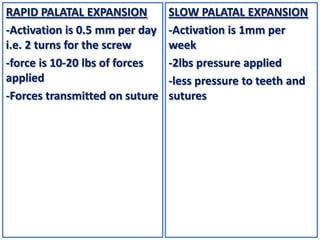
This document defines and describes different types of crossbites, including buccal, lingual, palatal, unilateral, bilateral, functional lateral, complete mandibular, complete maxillary, scissor bite, anterior, and posterior crossbites. It discusses the prevalence, etiology, diagnosis, and treatment of crossbites, which can include the use of inclined bite planes, rapid palatal expanders, and slow palatal expanders in younger patients, and transverse maxillary expansion in older patients. Left untreated, crossbites can cause complications like growth modifications, dental compensations, condylar deviation, and TMJ issues.