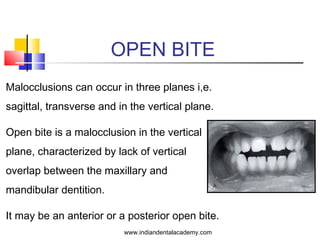









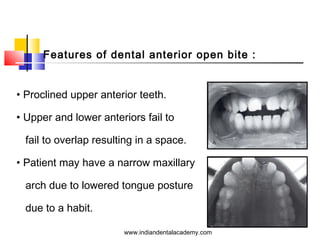












Open bite malocclusions can occur in the sagittal, transverse, and vertical planes, characterized by a lack of vertical overlap of dentition, with anterior and posterior types. Various hereditary and environmental factors contribute to their etiology, including thumb sucking and tongue thrusting, while clinical considerations include a range of open bite types and necessary therapeutic approaches. Treatment varies based on the malocclusion's localization and etiology, encompassing habit control, myofunctional appliances, orthodontics, and surgical correction.


































































































