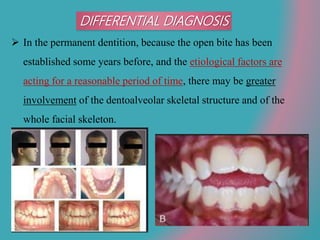
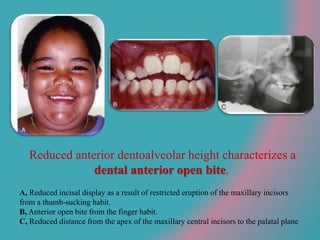
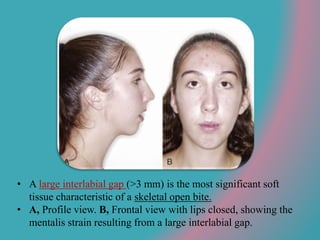
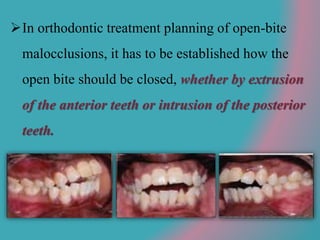
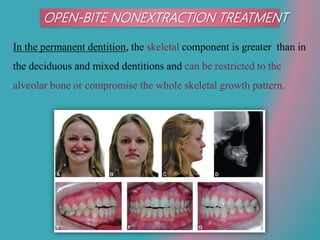
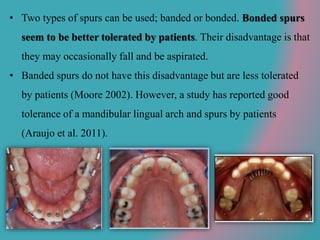
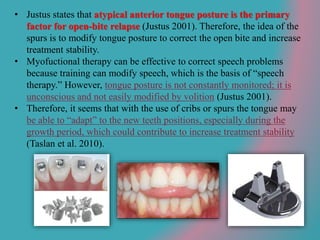
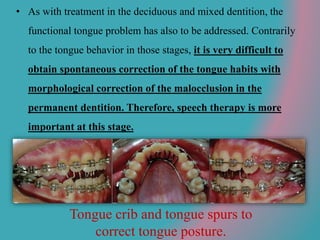
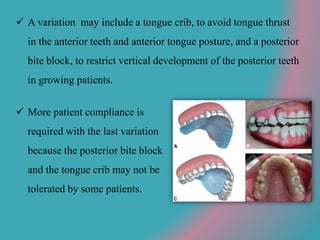
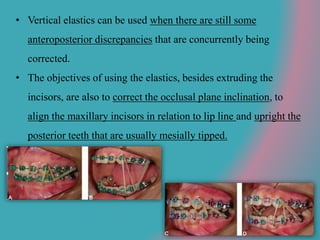
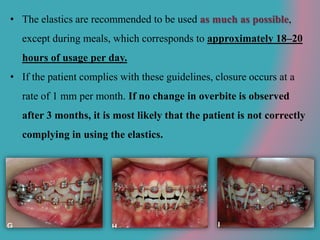
This document discusses open bite treatment in the permanent dentition using vertical elastics. It begins by differentiating between dentoalveolar and skeletal open bites, noting that skeletal open bites involve greater skeletal involvement and are more difficult to treat. Nonextraction treatment of open bites uses vertical elastics to extrude anterior teeth and close the bite over 18-20 hours per day. Tongue posture must also be addressed through the use of tongue cribs or spurs. Retention involves a maxillary retainer with an orifice to modify tongue posture. Close monitoring is needed to ensure patient compliance with elastic wear.



























































![FACEMASK CHINCUP SEMINAR[1].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/facemaskchincupseminar1-230916061625-e0964de8-thumbnail.jpg?width=640&height=640&fit=bounds)