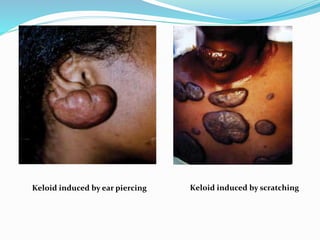
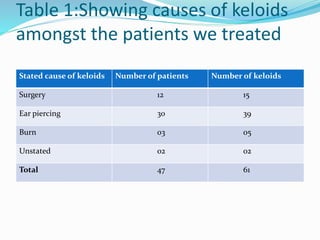
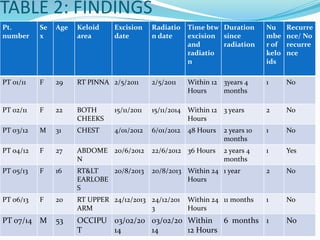
This document discusses keloids, which are benign scar tissue growths that can form after skin trauma. Keloids have a high recurrence rate after surgical removal alone. The document presents a study of 47 patients in Kenya with 61 keloids treated with surgical excision followed by a single dose of 9Gy electron beam radiation within 24 hours. Two keloids recurred, both in patients treated over 24 hours after excision. The summary concludes immediate post-operative radiation after keloid excision is effective for preventing recurrence.




































































































![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)









![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)