Response To Injury
•Wound healing
– An organism’s global response to injury, regardless
of the location of injury.
– Progression from injury to stable scar
• Common Features
Wound Healing
• ProliferativePhase: days 4-21
– Granulation tissue: fibroblasts, macrophages, &
endothelial cells.
– Collagen
– Endothelial cells
• As important as this phase of wound healing is
there comes a point where it needs to cease
8.
Wound Healing
• RemodelingPhase: 21 days up to 1 year
• Wound contraction & collagen remodeling
– Myofibroblasts
– Collagen
10.
Abnormal Response &Healing
• Balance between regeneration and Scar
formation
• Inadequacy in regeneration
• Inadequate Scar Formation
Excessive Scar Formation
•Abnormal scarring of the skin
– Keloid: <6% of population primarily affecting black
and Asian populations
• Thick collagen fibers composed of numerous fibrils
closely packed together
– Hypertrophic Scars
• Near universal outcome following extensive deep burn
injury
Epidemiology
• Keloids occurequally across gender
– More common in younger individuals of African,
Asian, & Hispanic descent
– Heritability
• HTS incidence higher in persons 10- 30 years
old
Prevention cont..
• Siliconesheeting
• Scar reduction from silicone occurs through
– Oclusion and hydration of outer layer of
epidermis, generation of static electricity, and a
reduction in mast cells
• Start 2 weeks after primary wound treatment,
leave on as much as possible per day for a
minimum of 2 months
23.
Prevention Cont..
• PaperTapes
– Placement over incision lines
• Flavonoids
• Hydration with emollient
• Scar Massage
Injectable
• Intralesional Corticosteroids
–Anti-inflammatory, ant-proliferative,,
immunosuppressive, and vasoconstrictive
properties
– Triamcinolone 10-40 mg/ml every 4-6 weeks
• 5FU
– Intralesional can be combined with corticosteroids
• Bleomycin: cytotoxic antibiotic with antiviral,
antineoplastic, and antibacterial properties
27.
Surgical Therapies
• Cryotherapy:topical or intralesional
– Recurrence uncommon & depigmentation is
temporary
• Freeze thaw cycles between 10-20 seconds
28.
Modified Vancouver ScarScale
Vascularity Pliability Pain
Normal 0 Normal 0 None 0
Pink 1 Supple 1 Occasional 1
Red 2 Yielding 2 Requiring
medication
2
Purple 3 Firm 3 Pruritus
Pigmentation Ropes 4 None 0
Normal 0 Contracture 5 Occasional 1
Hypopigment
ation
1 Height Requiring
medication
2
Flat 0 Total Score Out of 16
< 2 mm 1
Mixed 2 2-5 mm 2
Hyperpigmen
tation
3 > 5 mm 3
29.
Surgical Revision
• Indication
–Note: Scars take 12-18 months in order to mature
• Contraindications
– Cases where new scar will be worse
– Working with a mental health professional
• Timing
Principles of TissueRearrangement
• Guided by same principles as prevention
• Restoration of anatomic landmarks
• Reorientation of scars
• Scar elongation & irregularization
33.
Scar Revision Techniques
•Z-plasty
– 4 fundamental functions: length, breaking up a
line, moving tissue, & obliterating or creating a
web or cleft
38.
Postoperative Care &Follow-up
• Optimize wound healing
– Adequate nutrition
– Blood sugar control
– Smoking cessation
– Activity precautions
• Tension off-loading
• Long term follow-up
39.
Other Therapies
• LaserTherapy: 585 nm PDL ( most commonly used)
• Radiotherapy
– External beam, internal radiation, or with radioactive
skin patches
– Postoperative radiotherapy more effective than
radiotherapy alone at lowering recurrence of keloids
40.
Emerging/Experimental Therapies
• Botulinumtoxin A
– Induce paralysis of musculature surrounding scar
• Mesenchymal Stem Cell (MSC) therapy
– Release of growth factors
• Fat grafting
– Injection or fat tissue grafting underneath or into
the wound
• Interferon-α-2β
References
• Eun MeeOh, Y. C. (2013). Assessment of Postoperative
Scar Using Modified Vancouver Scar Scale of 283
Patients Who Underwent Open Thyroidectomy in a
Single Institution. Korean J Endocr Surg.
• Herndon, D. N. (2018). Total Burn Care 5th ed. .
London.
• Michael 2. Hu, E. R. (2018). Scar prevention , treatment,
and revision . In P. C. Neligan, Plastic Surgery Principles
(pp. 196-213). Toronto : Elsevier Inc. .
Atrophic scars
• Developas a result of intracutaneous
inflammatory process
– Results in reduced matrix regeneration and focally
reduced collagen production
– Focal contraction results in reduced uneven soft
tissue defects
• 3 clinical conditions present for reconstructive
management
– Acne, striae albae, and burns
45.
Atrophic scar mgmt
•Microdermabrasion
– Minimally invasive technique that improves texture
but only addresses superficial scars, combinaiton
with aminolevulinic acid photodynamic therapy is
more effective,
– Subsequent remodeling results in neocolangenesis
and hence increased dermal thickness
– Mainly for well-defined superfical scars with distinct
borders or broad mbsed scars with indistinct
borders
46.
Atrophic Scar mgmt
•Chemical Peels & microneedling
– Improve pigmentation, tone, & texture
– Potential adverse effects include prolonged erythema and post
inflammatory hyperpigmentation
– Side effects more prevalent but not limited to deep peels
– High concentrations of TCA high efficacy in atrophic scars
– Skin needling: based on principle of percutaneous induction of
collagen, creating dermal mircroclefts, with collagenases
resulting from cascade of growth factors unleashed by
wound0healing process
• More effective on rolling scars takes repeat sessions and up to a year
to be complete
47.
Atrophic Scar mgmt
•Punch Excision
– Converts a discrete atrophic scar into a well-apposed, well
oriented surgical healthy scar
– Full thickness excision
– Wound sutured along relaxed skin tension lines
– Avoid closely spaced defects & thus excess traction
– Punch excision replaced by sharp elliptical excision to avoid
standing cone formation, when defect larger than 3 mm
– Once healed, resulting surgical wounds can be
incorporated into laser remodeling
Editor's Notes
#4 Process of wounding activates systemic processes that alter physiology far beyond the confines of the defect itself. Inflammatory cascades that impact nearly every organ system and have potentially dire consequences for survival are initiated.
During this progression there is activation of clotting system, acute and chronic inflammatory response, neovascularization, angiogenesis & vasculogenesis, cell proliferation, ecm deposition and remodeling
All of these events occur simultaneously and interact and influence each other at the level of gene transcription and protein translation in a dynamic and continuous fashion
Wound healing is an organisms response to physical disruption of tissue/organ to re-establish homeostasis of that tissue/organ and stabilize physiology
#5 Reestablishment of tissue can occur by one of two processes
Scar formation: whereby substitution of a different cellular matrix a s a patch to immediately re-establish both a physical and physiologic continuity of the injured organ is achieved.
Regeneration: reactivation of developmental pathways occurs and architecture of the original organ is re-created.
Balance between these pathways differs from between different organs. Neural tissue has little regeneration and heals by scarring whereas bone and the liver heal primarily through regeneration
This also differs across species where some species like salamanders and axolotls are able to regenerate limbs
A rapid recruitment of inflammatory cells, and proliferative burst of activity to close a wound as quickly as possible reduced risk of invasive infection in a time where wound care and antibiotics were unavailable.
Tissue regeneration is not always beneficial consider peripheral nerve neuromas which are a dysfunctional attempt at regeneration of a damaged organ, which result in disabling condition. In this case scar formation would be preferred which is what ablation provides
#6 This phase begins immediately and aims to attain hemostasis, remove devitalized tissue, and prevent colonization & invasive infection by microbial pathogens
Clotting cascade activates to prevent hemorrhaging, while disrupted vessels allow circulating elements into the wound, platelets degranulate releasing growth factors PDGF and TGF-β. This matrix provides scaffolding for cell recruitment and attachment required during subsequent phases of wound healing
Over the first 2 days there is infiltration of neutrophils into fibrin matrix, they act to remove dead tissue by phagocytosis and prevent infection by O2 dependent and independent mechanisms. NB the persistent presence of neutrophils in wounds is a proposed mechanism by which acute wounds become non-healing chronic wounds
During the time period between 4872 hours monocyte/ macrophages follow nuetrophils circulating monocytes go into wound and become macrophages becoming the dominant cell type in a healing wound by day 3. Phagocytose debris and bacteria and are critical to production of growth factors necessary for production ecm by fibroblasts and for production of blood vessels
Absence of macrophages has sever consequences for healing wounds unlike the absence of neutrophil
Lymphocytes are the last cells to enter wound, having a less defined role but stimulatory population of CD4 and inhibitory CD8 cells precede the subsequent proliferative phase
#7 Phases of wound healing are not exclusive and have overlap, facets of proliferation like re-epithelization occur almost immediately following injury keratinocytes adjacent to wound alter phenotype, regression of desmosomal connections b/n keratinocytes and to underlying basement membrane frees cells and allows lateral migration
Provisional fibrin matrix gradually replaced by a new platform, granulation tissue is composed of 3 cell types that play critical role in granulation tissue formation. These cells form ECM and new blood vessels.
Granulation tissue begins to appear at 4th post injury day fibroblasts produce the ECM that fills healing scar and the scaffold for keratinocyte migration.
Provisional matrix of fibrin is replaced by thinner type III collagen which will be replaced by thicker type I collagen during remodeling phase
Endothelial cells are critical component of granulation tissue they for new blood vessels through angiogenesis and vasculogenesis (involves recruitment and assembly of bone marrow derived progenitor cells
Macrophages release pro angiogenic factors VEGF, FGF 2 angiopoietin 1, & thrombosopndin. Relative timing of these factors and importance is unclear but they are important for wound healing during this phase.
Formation of granulation tissue and ecm needs to be halted at a certain point in a regulated process, its activating process is not known but dysregulation of this process is believed to underlie fibrotic disorders such as hypertrophic scarring
#8 This is the longest component of wound healing once a wound is filled with granulation tissue and after kerationcyte migration has re-epitheliaized it process of wound remodeling occurs
Remodeling likely begins with regression of blood vessels and granulation tissue,
Contraction is produced by wound myofibroblasts which are fibroblasts with intracellular actin microfilaments, capable of force generation and matrix contraction
Contract the wound through integrin mediated cell matrix interactions with dermal environment
Collagen remodeling is characteristic of this phase Type III collagen that’s initially laid down by fibroblasts during proliferative phase is replaced by type I collagen over a period of weeks to months.
This process is mediated by matrix metalloprteinases secreted by macrophages, fibroblasts, and endothelial cells
During this stage breaking strenght of wounds improves due to collagen cell type turnover as well as collagen cross linking
At 3 weeks 20% of strength and at 1 year 70-80%
#10 Abnormal process in wound healing are a dynamic balance between these two forces in order to restore homeostasis at a cellular, tissue, organ level
Treatment is guided by the understanding of the underlying mechanism, where we would want regeneration to predominate for some scar tissues at other sites our preference would be for scar formation
In the central nervous system there is little if any capacity for neural regeneration and scar tissue replaces areas of damage
Potential targets are implantation of stem/prgenitor cells
Other examples of inadequacy of regeneration would be bony nonunion and corneal ulcers
Disease process results from failure to substitute tissue defect with patch of scar. Where a stable scar tissue would be adequate to restore continuity and eliminate pathology
Although regeneration of skin might be ideal its not required for the functional outcome: diabetic foot ulcers pressure sores, and venous stasis ulcers
Once the cause of the defect in scar formation is identified, therapeutic measures can be designed to correct these deficiencies
Identify where primary defect is occurring, during inflammatory, proliferative, or remodeling phase
#11 Pathways of regeneration lead to re-creation of absent tissue but with functional problems of reintegrating the tissue
Often occurring in peripheral nerve tissue i.e. neuroma, psoriasis, granuloma formation
Precancerous lesions as a result of over-exuberant attempts at tissue regeneration with disordered and uncontrolled growth
Therapy target in these cases would be decreasing cellular proliferation & blocking or impeding the aberrant regenerative pathways.
Example would be injection of alcohol into neuroma
#12 Abnormal scarring of the skin can be classified as either hypertrophic scarring or keloid formation both are a manifestation of oberexuberant scarring.
Keloids are differentiated by the overgrowth of dense fibrous tissue beyond borders of original wound
In contrast to keloids HTS doesn’t extend beyond original wound margins and are characterized by formation of dense fibrils following injury
More prone to forming disabiling contractures
Proposed mechanisms for these abnormal/excessive scarring: mechanical strain, inflammation, bacterial colonization, and foreign body reaction
#13 1. HTS Differs from normal skin and mature scar in several ways: 1 ECM is altered in composition and architecture, 2. keratinocytes and fibroblasts found in HTS are profibrotic, 3. Profibrotic cytokines are upreglated and with prolonged expression
Over time HTS undergoes remodeling and maturation leading to variation in its presentation, features of HTS are shared by other fibroproliferative disorders include: renal fibrosis, pulmonary fibrosis and scleroderma.
ECM in healing wounds is laid down by fibroblasts and subsequently remodeled as scar matures, ECM in HTS displays significant differences from mature scar and normal skin, notably arrangement and composition of collagen bundles and in relative proportions of proteoglycans.
#14 Provides scaffolding for cells and mechanical strength to tissues, in HTS quantity of collagen per unit surface area is increased however relative proportion of collagen in HTS is decreased compared to normal skin due to much greater increases in proteoglycans and glycoproteins
This composition of ECM in HTS alters collagen fibrils, making the thinner and disorganized
Normal wound healing type III collagen appears early then gradually disappears as the scar is remodeled and matures which doesn’t occur in HTS
Other alterations occurring hts beyond fibrilar composition and morphology is alteration in interfibrialr spacing which is irregular and increased, with the space filled by proteoglycans and glycoproteins
#15 Turgor, resilience, & resistance to compression
Formed by a protein core, with repeating units such as leucin in decorin and glycosaminoglycan side chains which are ionized and hydrophilic making them mainly responsible for tissue water retention.
2. Glycoproteins like fibronectin are generally involved in cell-matrix adhesion and influence cell behavior by this mechanism
#16 Diagnosed clinically, HTS generally appears within 1 month of injury & grow over a 6 month period, but can regress within 1 year or stabilize
HTS contained within boundaries of original injury, and typically occur in areas of high tension
Keloids arise within 3-12 months following cutaneous trauma in predisposed individuals
#18 4-16% incidence among Black and Hispanic populations, in Caucasians <1%
Family heritability, & prevalence in twins suggests a genetic predisposition to keloids
Inheritance is autosomal dominant with incomplete clinical penetrance and variable expression other reports autosomal recessive and X-liked inheritance
They can occur up to 91% of the time following burns in those with ful thickness burns HTS prevalence is up to 70%
#19 Current strategies focus on the reduction of inflammation,
Minimizing tension is the single most important modifiable factor in the prevention of scar formation. When greater tension is applied at the edges of a wound, excessive scarring is more likely to occur
Complete mechanism is still unclear but by reducing mechanotransduction there is likely a reduction in the associated activation of the inflammatory response
Use of pressure garments, bandages, adhesive plaster molds, or specialized devices, have previously been found to minimize scarring.
Results in attenuated release of inflammatory cytokines and reduction in collagen synthesis and scar formation
Also thought to increase apoptosis, decrease angiogenesis contributing to reduction in pathologic scar formation
#20 Utilize fine instruments, and atraumatic techniques to minimize trauma to tissue using hooks instead of double grasping with forceps
Relieve tension on apposed epidermal edges, wound tension causes edge separation and scar widening with time, approximate tissue with
deep buried subdermal stiches
Gillies near far pulley can be used to aid approximation of higher tension tissue
Skin eversionis an exaggeration of tension free principle
Place sutures at wound periphery work redundancy towards the middle
More superficial bite of thicker tissue and deeper bite of thicker tissue
#21 Use fine sutures for closure and promptly remove ie on face 3-5 days and if necessary use adhesive strips to reinforce at time of removal
Or use of subcuticular sutures permanent sutures like prolene or nylon incite less reaction than absorbable biodegradable sutures either tape the ends or externalize at intervals to make removal easier
Placement along these lines has 2 benefits: scar is parallel or within a natural crease which will camouflage it and location also places least amount of tension on the wound
#22 Provides passive mechanical stabilization, mitigates the growth potential of the scar & encourage normal healing
Soft, self-adhesive, and semiocclusive sheet containing medical grade silicone reinforced on a silicone membrane backing.
Areas where its difficult to apply sheets silicone gel can be used
#23 Reduce tension on wound edges & minimizing shearing
Compounds obtained from plants with interest in management of scars due to anti-inflammatory properties. Alium cepa an extract from onions is shown to have anti-inflammatory properties
Quercetin (found in plants) shown to inhibit fibroblast proliferation, collagen production, and contraction of keloid, and HTS derived fibroblasts.
Petrolatum and application of sunscreen, avoiding sun or sunscreen with high protection factor protect from UV exposure which is shown to increase scar pigmentation
Decrease scar-related pain and itchiness, no studies have successfully demonstrated its effectiveness of HTS prevention
#25 As in prevention these methods can also be used as therapy being one of the first lines of therapies for HTS & Keloids having modest but inconsistent efficacy
Toll like receptor immune response modifier; conflicting result with some reports demonstrating improvement when cream is applied daily or on alternate days
Verapamil a ccb stimulates enzyme collagenase which increases degradation and prevents production of collagen, effective in 2 randomized control trials. With one demonstrating that it may be as effective as Intralesional Corticosteroid but with fewer side effects
#26 Often done in combination with silicone sheeting.
Help reduce pain and pruritus, reduce collagen & glycosaminoglycan synthesis, inhibit fibroblast proliferation, & cause degeneration of collagen, and fibroblasts
Intralesional administration attains higher concentrations at scar site with minimal systemic absorption
Typically systemic side effects are not seen since low doses are used but can be associated with htn, heart failure, uncontrolled dm, and bacterial/fungal infections
Pyrimidine analog that inhibits thymidylate synthase enzyme: inhibits fibroblast proliferation, induces fibroblast apoptosis without necrosis, delays cell cycle progression, & inhibits TGF-β induced collagen type I synthesis
Mechanism of action is still unknown but it is shown to decrease collagen synthesis, reduces lysl-oxidase levles, and can induce apoptosis
#27 Shown to be effective for small keloids and HTS, liquid nitrogen can be delivered externally (contact or spray) or via an intralesional needle cryoprobe
Intralesional is the most efficacious form of cryotherapy: following single session patents saw a 51.4% reduction in scar volume and required less treatment cycles overall, following second session 30-75% of keloids improved with higher rates seen in HTS
Technique is safe associated with depigmentation, recurrence, and pain
External method associated with hypopigmentation, blistering, pain delayed healing, and infection, with larger scars requiring repeated sessions.
Cryotherapy works by inducing cell injury and necrosis in the treatment area
Surgical excision, to reduce or remove scar; not recommended unless conservative therapies are not successful or do not provide significant improvement.
Recurrence rates are low in HTS but for ekoid rates vary 45-100% combination with other therapies can reduce the rates.
#28 1. Surgical treatment is based on analysis of a scar’s characteristics: morphology, maturity, distortion of tissues and appropriate application of non-invasive measures
#29 Patients seek revision for many reasons that include physical and psychological reasons
Functional limitations due to location across mobile areas or lack of tissue laxity causing contractions
Pain: scars can also be painful especially if a neuroma is present so excision or repair of neuroma is an important component
Traumatic reminder/ or causing social embarrassment
NB operating on non mature scars will have poor outcome
Unrealistic expectations: scar revision is to improve or create a more acceptable scar not to eliminate
Immature scars contain fragile blood vessels of neovascuaraization and will bleed in excess, a tissue which is primed for revision is maximally mobile and soft , so clinical examination is important
#30 Single stage can range from simple direct excisions to complex soft tissue rearrangements
Preop suturing and on table tissue expansion can be used to decrease tension on wound after direct excision
Undermining and advancement of skin edges also allows for re-approximation without tension
Serial excision is circumferentially excising the scar margin undermining and advancing bordering normal tissue
Pliability of surrounding tissue should be assessed to determine how much scar is safe to excise
Tissue expansion placement of expander beneath the skin to grow extra skin for use in reconstruction
#31 Scarring occurs in 3 dimensions and extends to deeper tissues; this process can result in puckering and tethering of overlying tissue
Can occur in absence of superficial injury
After release the defect sometimes requires interposition of muscle or fascia
Procedures using lasers or chemical peels can even out contour deformities
For those having more severe scarring focal excision with tethered tissue release is more effective
#32 Atraumatic technique, tensionless closure & proper skin eversion
Landmarks such as vermillion border, eye position or alar base should take priority over minimizing scar characteristics
Use of local flaps in the face to prevent distortion is an example of this, so larger scar of flap is preferred when local tissue recruitment would result in deformity of facial landmarks
Reorientation of scars to Langer’s lines allows for least tension across a wound
At rest scars may become less visible but scars in the face may become more apparent with expression
Myofibroblasts in a mature scar can cause contracture within the axis of the scar, a long, straight scar will result in uniform contracture in one axis causing greater deformity in the surrounding tissue and greater depression of the scar.
This can lead to limitations of movement, and change in contour may be aesthetically unpleasant
Thus reorientation and rearrangement techniques break up the length of ascar by incorporating neighboring tissue
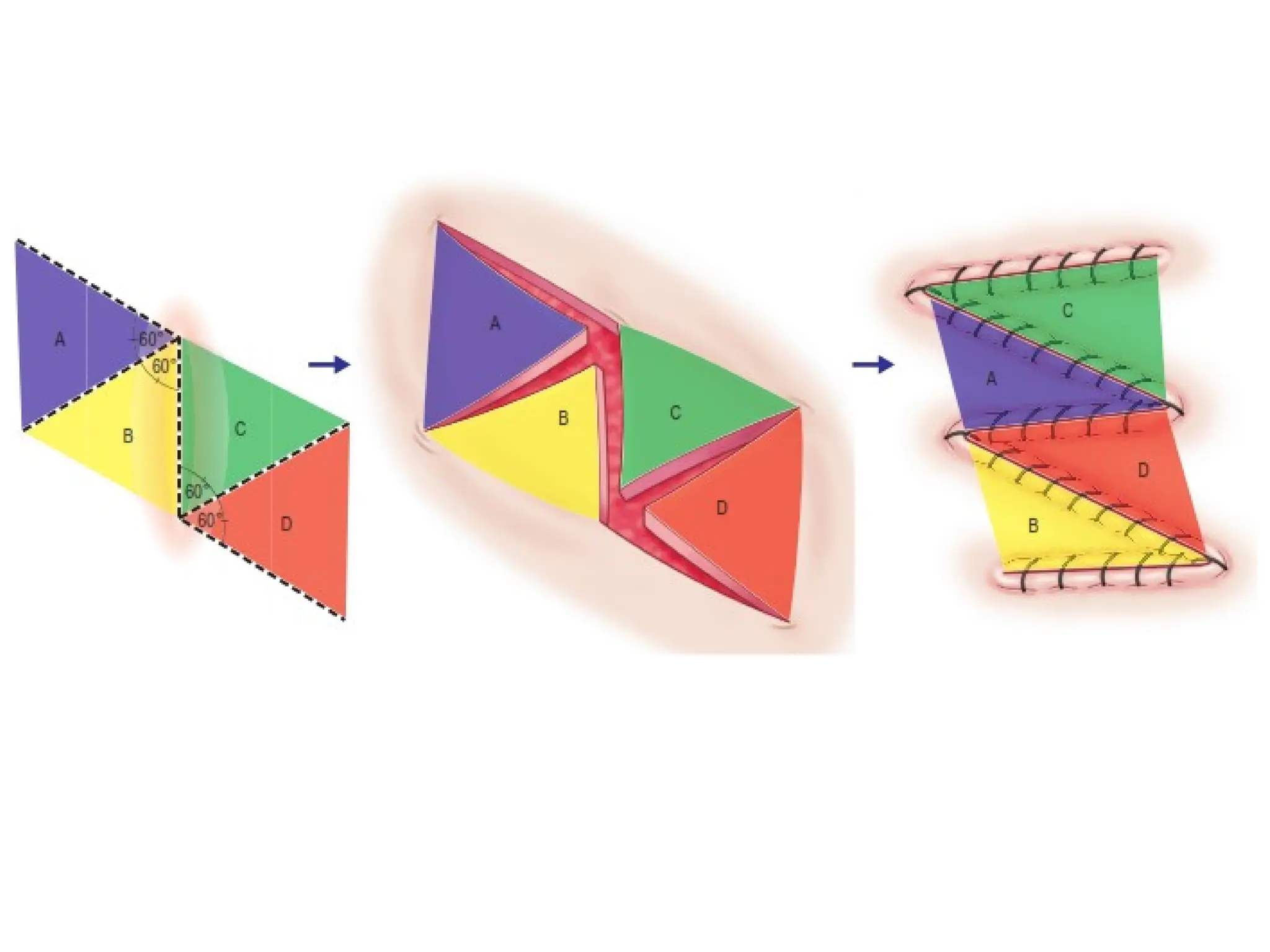
#33 Transposition of two triangular flaps, usually of equal size and equal angle into each others defect
Theoretical gains achievable with changes in the angle of the lateral limbs, in practical terms elasticity of skin and rigidity of scar create unequal deformation off central and lateral limbs so gains in length in vivo is less than expected
Z plasties are divided into: simple, planimetric, skew, & multiple
#36 Planimetric z-plasty is a variation of the classic z-plasty, it maintains the flaps in the same plane, it minimizes amount of rotation and excises redundant tissue, it avoids contours and depressions created by simple z-plasty.
May be designed with lateral limb angles ranging from 60-90 degrees but most often planned at 75 degrees
Ideal for scar releases on flat surfaces where lengthening is the primary objective and contour deformities would be suboptimal
#37 1.Multiple Flap z-plasties: refers to multiple Z-plasties along a scar length as well as z-plasties designed with more than 2 flaps
1. when multiple plasties are performed in a series, the previous Z-plasty exerts deformational forces on the tissue of the next z-plasty further limiting actual gain in length
2. A single large Z-plasty, however is not always in keeping with aesthetic and functional goals of a scar revision
3. Widen tips of flaps to avoid tip necrosis
4. The thickness of flaps is dictated by the quality and location of the tissue, scars often have distorted with unreliable blood supply, therefore thicker flaps are necessary.
in unscarred tissue, care must be taken to elevate the subdermal vascular plexus to include the cutaneous microvasculature in the flap
1. Other techniques include V-Y and Y-V advancement flaps, W-Plasty, and geometric broken lines
#38 1. Taping, silicone sheeting, compression, and scar massage may provide modest improvement
#39 A 2nd or 3rd line option in treatment of HTS and keloids following failure of silicone sheeting or Intralesional steroids.
PDL, fractional CO2, ER:: YAG 2940 nm, & Er-doped laser 1550nm
Improvement in scar erythema height & pliability seen
Drawback is that in susceptible areas: head, neck and breast in under 18 patients there is increased risk of carcinogenesis
Induces antiangigenic and anti-inflammatory properties.
24-48 hours postop across several sessions with total recommended dose of 40 grays.
#40 Intralesional injection of toxin
Relaxation of the muscle decreases tension
Intralesional injections: reduced size of keloids as well as no reappearance of lesion or symptom at 1 year follow-up and high patient satisfaction and administration for HTS patients also showed acceptable improvement, erythema, itching sensation & pliability scores significantly reduced compared to pretreatment
When administered with triamcinolone or postexcision of keloids has demonstrated significant decrease in volume, depth, as well as reduced recurrence rates, compared with controls.
Drawback significant dropout rates due to injection site pain and flulike symptoms associated with interferon
Through release of growth factors (MSCs) can modulate inflammatory responses and have an antifibrotic effect
Local injection, systemic, or use of MSC seeded tissue scaffold,
Improvement in macroscopic and histological appearances of scars
Theory: adipose derived stem cells, possess biological properties that improve cutaneous fibrosis, in part related to angiogenic and anti-apoptotic properties
ASC able to regulate vessel density, collagen, thickness, and granulation process which all can lead to improved appearance of scars