Download as PDF, PPTX


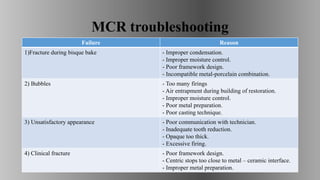


The document discusses dental porcelain, outlining its definition, history, properties, types, uses, and advantages/disadvantages. It details how dental ceramics, particularly porcelain, have evolved since the late 19th century, including key developments like the introduction of porcelain-fused-to-metal crowns and advancements in all-ceramic restorations. Additionally, it addresses troubleshooting for metal-ceramic restorations, highlighting common failure reasons and their solutions.





























































![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)





![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)