Ceramic-
An inorganic, nonmetallicmaterial composed of metallic or semi-metallic
oxides, phosphates, sulfates, or other nonorganic compounds.
Dental porcelain-
A ceramic produced by sintering a mixture of feldspar, silica, alumina, other
metal oxides, pigments and opacifying agents. Except for porcelain denture
teeth, dental porcelain is not made from kaolin.
INTRODUCTION
5.
• Ceramics aremore resistant to corrosion than plastics.
• Do not react readily with most liquids, gases, alkalis and weak acids.
• Remain stable over long time periods.
• Excellent thermal and electric insulators.
PROPERTIES
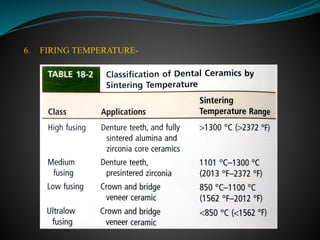
6.
• Good toexcellent strength and fracture toughness.
• Esthetic
• Biocompatible
• Wear resistant
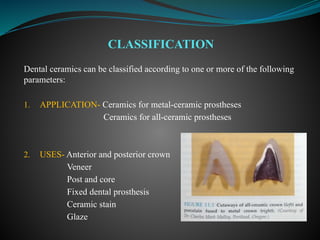
Dental ceramics canbe classified according to one or more of the following
parameters:
1. APPLICATION- Ceramics for metal-ceramic prostheses
Ceramics for all-ceramic prostheses
2. USES- Anterior and posterior crown
Veneer
Post and core
Fixed dental prosthesis
Ceramic stain
Glaze
CLASSIFICATION
1. Powder/liquid, glass-basedsystems
2. Machinable or pressable blocks of glass-based systems
3. CAD/CAM or slurry, die-processed, mostly crystalline (alumina or
zirconia) systems.
Shenoy A, Shenoy N. Dental Ceramics: An update. JCD 2010;13(4):196.
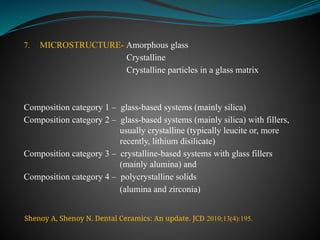
7. MICROSTRUCTURE- Amorphousglass
Crystalline
Crystalline particles in a glass matrix
Composition category 1 – glass-based systems (mainly silica)
Composition category 2 – glass-based systems (mainly silica) with fillers,
usually crystalline (typically leucite or, more
recently, lithium disilicate)
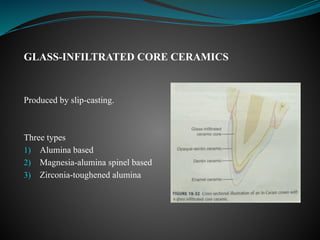
Composition category 3 – crystalline-based systems with glass fillers
(mainly alumina) and
Composition category 4 – polycrystalline solids
(alumina and zirconia)
Shenoy A, Shenoy N. Dental Ceramics: An update. JCD 2010;13(4):195.
• Metal-ceramic crownsand fixed partial prostheses
• All-ceramic crowns, inlays, onlays and veneers
• Denture teeth
APPLICATIONS OF CERAMICS IN DENTISTRY
17.
In approx. 700B.C, the Etruscans made artificial teeth of ivory and bone
that were held in place by gold wires or flat bands and rivets.
Animal bone and ivory from hippopotamus were used for many years
therafter.
HISTORY
18.
First sets ofdentures were made for US President George Washington which
contained extracted teeth but later his dentures were made of hippopotamus
ivory.
The ivory tooth forms were supported in the maxillary denture by a gold palatal
plate and the dentures were retained by pressure applied by coiled springs
attached to the sides of denture bases.
19.
The use ofmineral teeth or porcelain dentures greatly accelerated an end to
the use of human and animal teeth.
Feldspathic dental porcelain was adapted from European triaxial white ware
formulations (clay–quartz–feldspar).
In 1723, enameling of denture metal bases was described by Pierre Fauchard
in Le Chirur Gien Dentisle.
The first porcelain tooth material was patented in 1789 by a French dentist
(de Chemant) in collaboration with a French pharmacist (Duchateau).
20.
This material wasan improved version of “mineral paste teeth” produced in
1774 by Duchateau.
It was introduced in England soon thereafter by de Chemant.
In 1808, Fonzi, an Italian dentist, invented a “terrometallic” porcelain tooth
that was held in place by a platinum pin or frame.
Planteau, a French dentist, introduced porcelain teeth to the United States in
1817 and Peale, an artist, developed a baking process in Philadelphia for
these teeth in 1822.
21.
Commercial production ofthese teeth began in 1825 by Stockton.
In England, Ash developed an improved version of the porcelain tooth in
1837.
In 1844, the nephew of Stockton founded the S.S. White Company, and this
led to further refinement of the design and the mass production of porcelain
denture teeth.
22.
Glass inlays (notporcelain) were introduced by Herbst in 1882 with crushed
glass frit fired molds made of plaster and asbestos.
In 1885, Logan resolved the retention problem encountered between
porcelain crowns and posts that were commonly made up of wood by fusing
the porcelain to platinum post-Richmond crown. These crowns represent the
first innovative use of the metal ceramic system.
In 1886, combining the burnished platinum foil as a substructure with the
high controlled heat of a gas furnace, Dr. Land introduced first fused
feldspathic porcelain inlays and crowns.
23.
Dr. Charles Landintroduced one of the first ceramic crowns to dentistry in 1903.
A noteworthy development occurred in 1950 with an addition of leucite to
porcelain formulation that elevated the coefficient of thermal expansion to allow
fusion to certain gold alloys to form complete crowns and FPD.
The first commercial porcelain was developed by VITA Zahnfabrik in 1963.
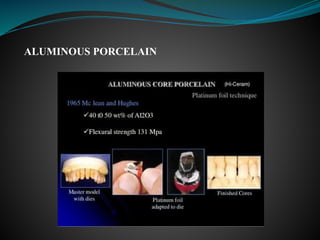
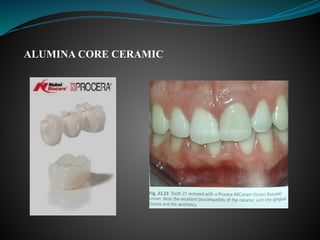
In 1965, McLean and Hughes developed a Porcelain Jacket Crown (PJC) with an
inner core of aluminous porcelain containing 40–50% alumina crystals to block
the propagation of cracks.
24.
Adair and Grossman(1984) demonstrated an improvement in all-ceramic
systems developed by controlled crystallization of a glass (Dicor).
In early 1990s, a pressable glass glass-ceramic (IPS Empress) containing
approximately 34% leucite by volume was introduced.
A more fracture resistant, pressable glass-ceramic (IPS Empress 2)
containing approximately 70% lithia disilicate crystals by volume was
introduced in late 1990s. This product could be used for 3-unit FPDs upto
second premolar.
25.
The CEREC 1system was introduced in the mid-1980s, and improvements
in software led to the CEREC 2 and CEREC 3 systems for the production of
ceramic inlays, onlays, and veneers.
In 1992, Duracem LFC (low-fusing ceramic) was marketed as an ultralow-
fusing ceramic.
26.
• Anusavice, Shen,Rawls. Phillips’ Science of Dental Materials.
Elsevier.2013;12edi.
• Powers JM, Sakaguchi RL. Craig’s Restorative Dental Materials.
Elsevier.2006;13edi.
• Shenoy A, Shenoy N. Dental Ceramics: An update. JCD
2010;13(4):195-196.
• Krishna JV, Kumar VS, Savadi RC. Evolution of metal-free ceramics.
JIPS 2009;9(2):70-71.
REFERENCES
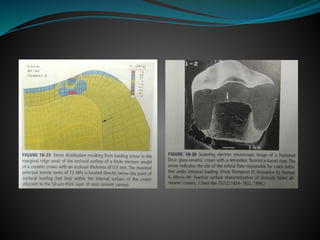
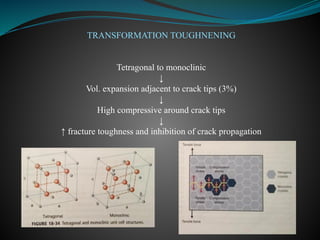
METHODS OF STRENGTHENINGCERAMICS
1) MINIMIZE THE EFFECT OF STRESS CONCENTRATIONS
Stress raisers are discontinuities in ceramic and metal-ceramic structures
that cause a stress concentration in these areas.
Abrupt changes in shape or thickness in the ceramic contour can act as
stress raisers and make the restoration prone to failure.
For eg, the incisal line angles on an anterior tooth prepared for a ceramic
crown should be well rounded.
31.
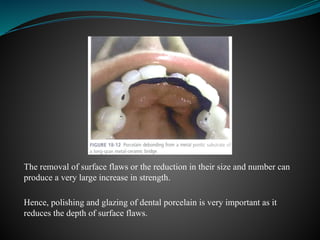
The removal ofsurface flaws or the reduction in their size and number can
produce a very large increase in strength.
Hence, polishing and glazing of dental porcelain is very important as it
reduces the depth of surface flaws.
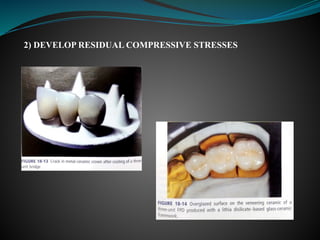
One method ofintroducing compressive stresses is to choose veneering
ceramics whose CTE or CTC is slightly less than that of core ceramic.
The same principle can be applied to metal-ceramic system.
The metal and porcelain should be selected with a slight mismatch in their
thermal contraction coefficients (the metal thermal contraction coefficient
being larger) so that the metal contracts slightly more than the porcelain on
cooling from the firing temperature to room temperature.
This mismatch leaves the porcelain in residual compression and provides
additional strength for the prosthesis.
34.
3) MINIMIZE THENUMBER OF FIRING CYCLES
Increased no. of firing cycles
Increased conc. of leucite
Increased CTC/CTE
Increased stresses
Immediate or delayed crack formation
35.
4) ION EXCHANGE
Theion exchange process is sometimes called chemical tempering and
involves the sodium ion since sodium is a common constituent of a variety
of glasses and has a relatively small ionic diameter.
If a sodium containing glass article is placed in a bath of molten potassium
nitrate, potassium ions in the bath exchange places with some of the sodium
ions in the surface of the glass article and remain in place after cooling.
Since the potassium ion is about 35% larger than the sodium ion, the
squeezing of the potassium ion into the place formerly occupied by the
sodium ion creates very large residual compressive stresses.
36.
5) THERMAL TEMPERING
Thermaltempering creates residual surface compressive stresses by rapidly
cooling (quenching) the surface of the object while it is hot and in the
softened (molten) state.
This rapid cooling produces a skin of rigid glass surrounding a soft (molten)
core.
As the molten core solidifies, it tends to shrink, but the outer skin remains
rigid.
The pull of the solidifying molten core, as it shrinks, creates residual tensile
stresses in the core and residual compressive stresses within the outer
surface.
37.
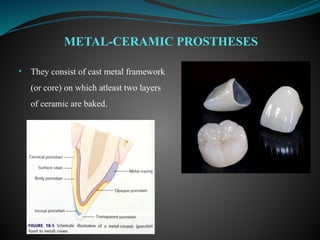
• They consistof cast metal framework
(or core) on which atleast two layers
of ceramic are baked.
METAL-CERAMIC PROSTHESES
38.
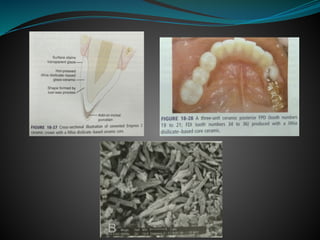
• The firstlayer applied is the opaque layer followed by buildup of
dentin and enamel porcelains.
39.
• The alloymust have high melting temperature.
• The veneering porcelain must have a low fusing temperature.
• The porcelain must wet the alloy.
• There should be good bond between ceramic and metal.
REQUIREMENTS FOR A METAL-CERAMIC
SYSTEM
40.
• CTE ofporcelain and metal should be compatible.
• Metal framework should have adequate strength and stiffness.
• High resistance to deformation is essential at high temperature.
• The tooth preparation must have adequate design.
41.
• Resistance tofracture.
• Less tooth structure needs to be removed to provide proper bulk for
crown.
• More esthetic compared to all-metal prostheses.
BENEFITS AND DRAWBACKS
42.
• Metal allergy.
•A dark line at facial margin associated with a metal collar when gingival
recession occurs.
43.
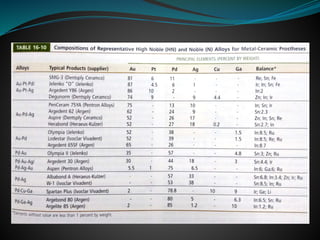
• Conventional dentalporcelain is a vitreous ceramic based on a silica
network (SiO2) and potash feldspar (K2O.Al2O3.6SiO2),soda feldspar
(Na2O.Al2O3.6SiO2) or both.
• Pigments, opacifiers and glasses are added to control the fusion
temperature, sintering temperature, coefficient of thermal contraction
and solubility.
CERAMIC COMPOSITION
44.
• Feldspathic porcelainscontain, by weight,
1. SiO2 matrix (52-65%)
2. Al2O3 (11-20%)
3. K2O (10-15%)
4. Na2O (4-15%)
5. Additives including B2O3, CeO2, Li2O, TiO2 and Y2O3
• Ultralow-fusing ceramicscontain less Al2O3 and increased
concentrations of CaO, K2O, Li2O and Na2O.
• They contain ,by weight, 20.1% to 22.6% tetragonal leucite and 0% to
2.6% cubic leucite.
• The conventional frits have been reported to be admixtures of three
kinds of glass frits. One of these ultralow-fusing frits exhibits very small
(less than 1) leucite crystals.
ULTRALOW-FUSING CERAMICS FOR
METAL-CERAMIC PROSTHESES
49.
• Ultralow-fusing enameland dentin ceramics may be easier to polish and
may yield smoother and less abrasive surfaces than conventional low-
fusing and medium-fusing porcelains.
• They have lower coefficients of thermal expansion and contraction
because of their lower concentration of leucite crystals compared with
conventional porcelains.
• They are compatible for use with alloys such as type II and IV gold
alloys that have lower fusion temperatures because of their lower
sintering temperatures.
50.
Effects of glassmodifiers:
• Increased fluidity(decreased viscosity)
• Lower softening temperature
• Increased thermal expansion
Disadvantages:
• Modifier conc. too high chemical durability of glass
• Glass may crystallize(devitrify) during firing if too many tetrahedra are
disrupted.
GLASS MODIFIERS
51.
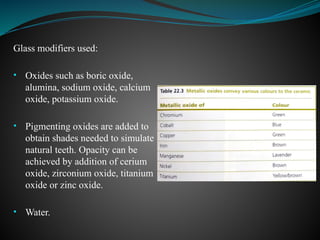
Glass modifiers used:
•Oxides such as boric oxide,
alumina, sodium oxide, calcium
oxide, potassium oxide.
• Pigmenting oxides are added to
obtain shades needed to simulate
natural teeth. Opacity can be
achieved by addition of cerium
oxide, zirconium oxide, titanium
oxide or zinc oxide.
• Water.
52.
PORCELAIN CONDENSATION
Dense packingprovides two benefits:
1. Lower firing shrinkage
2. Less porosity in the fired porcelain
FABRICATION OF METAL-CERAMIC
PROSTHESES
53.
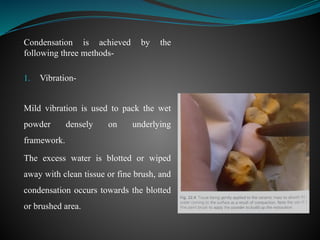
Condensation is achievedby the
following three methods-
1. Vibration-
Mild vibration is used to pack the wet
powder densely on underlying
framework.
The excess water is blotted or wiped
away with clean tissue or fine brush, and
condensation occurs towards the blotted
or brushed area.
54.
2. Spatulation-
A smallspatula is used to apply and smooth the wet porcelain.
The smoothing action brings the excess water to the surface, where it is
removed.
55.
3. Brush technique-
Thistechnique employs the addition of dry porcelain powder to the surface
to absorb the water.
The dry powder is placed by a brush to the side opposite from an increment
of wet porcelain.
As the water is drawn towards the dry powder, the wet particles are pulled
together.
56.
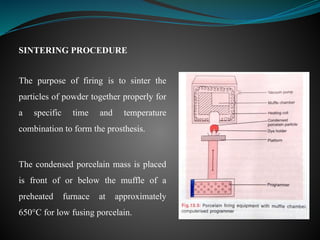
SINTERING PROCEDURE
The purposeof firing is to sinter the
particles of powder together properly for
a specific time and temperature
combination to form the prosthesis.
The condensed porcelain mass is placed
is front of or below the muffle of a
preheated furnace at approximately
650°C for low fusing porcelain.
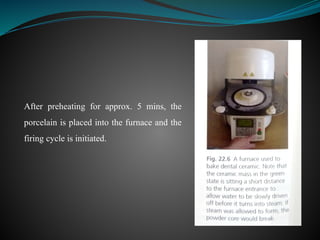
57.
After preheating forapprox. 5 mins, the
porcelain is placed into the furnace and the
firing cycle is initiated.
58.
Place porcelain infurnace
Pressure reduced to 1/10th
in the furnace causing air around the particles to
reduce to same pressure
Increase in temp.
Sintering of particles together and formation of closed pores
Vacuum released at a temp. which is 55°C below the sintering temp.
Increase in pressure from 0.1 to 1 atm
Pores compressed to 1/10th
of their original size
Total vol. of porosity reduced
CAST METAL COPINGSAND FRAMEWORKS
Copings and frameworks are produced by
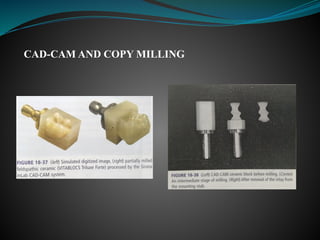
1. Casting of molten metal
2. CAD-CAM machining
3. Electrolytic deposition techniques
4. Swaged metal process
TECHNICALASPECTS OF METAL CERAMIC
PRODUCTS
61.
Phosphate bonded investmentmust be used.
Casting should be clean.
Framework for metal-ceramic bridges must not be deformed at porcelain
sintering temperatures.
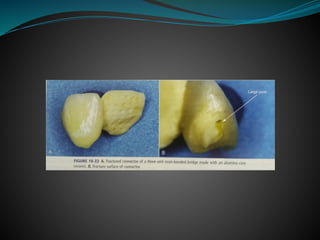
Connectors should be large enough to resist flexural strains that may cause
cracking under intraoral loading.
62.
CREEP OR SAG
Thecreep can be reduced if the metal has the proper composition so that a
dispersion strengthening effect occurs at high temperature.
The solidus temperature (the lower end of the melting range) of base metal
alloys, such as nickel-chromium is higher than that of gold alloys.
High temperature creep or sag of some high noble and noble alloys occurs
when the temperature approaches 980°C.
Once the alloy temperature decreases by 100°C or more, creep deformation
does not occur.
63.
CROWNS AND BRIDGESBASED ON SWAGED METAL FOIL
LAMINATES
Most widely used product- CAPTEK
It is a laminated gold alloy foil sold as a metal strip.
64.
This technology isbased on the principle of capillary action to produce a
gold-based composite metal.
Maximum span length for Captek-porcelain bridges- 18mm ( space upto
two pontics)
Thickness- 0.25mm (thinner than those produced by cast-metal process)
65.
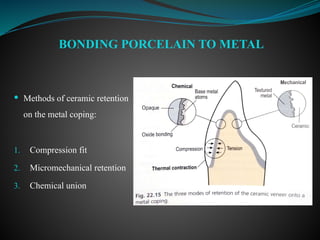
Methods ofceramic retention
on the metal coping:
1. Compression fit
2. Micromechanical retention
3. Chemical union
BONDING PORCELAIN TO METAL
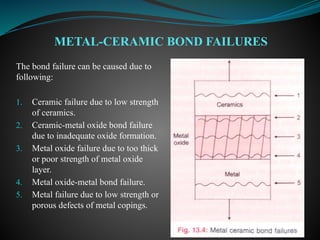
66.
The bond failurecan be caused due to
following:
1. Ceramic failure due to low strength
of ceramics.
2. Ceramic-metal oxide bond failure
due to inadequate oxide formation.
3. Metal oxide failure due to too thick
or poor strength of metal oxide
layer.
4. Metal oxide-metal bond failure.
5. Metal failure due to low strength or
porous defects of metal copings.
METAL-CERAMIC BOND FAILURES
67.
• Anusavice, Shen,Rawls. Phillips’ Science of Dental Materials.
Elsevier.2013;12edi.
• Powers JM, Sakaguchi RL. Craig’s Restorative Dental Materials.
Elsevier.2006;13edi.
• Bonsor SJ, Pearson GJ. A clinical guide to applied dental materials.
Elsevier.2013.
• Bhat VS, Nandish BT. Science of Dental Materials clinical application.
CBS Publishers and Distributors.2013;2edi.
REFERENCES
Advantages:
1) Improved aesthetics.
2)Increased flexural strength (because of higher crystalline content).
3) Enhanced fracture toughness.
Disadvantages:
1) Low translucency (due to presence of second phase in glassy matrix).
2) Increased sintering shrinkage.
3) Strength is inadequate for use in posterior teeth.
4) Fit is poor as compared to PFM.
5) Technique sensitive.
GLASS-CERAMICS
Glass ceramic wasfirst used in dentistry by MacCulloch in 1968.
The first commercially available castable ceramic material for dental use,
Dicor, was developed by Corning Glass Works and marketed by Dentsply
International.
Used as inlay, facial veneer and full crown.
77.
Dicor glass-ceramic containsabout 55 vol% of tetrasilicic fluormica
crystals.
Dicor MGC is a higher quality product provided as CAD-CAM blanks or
ingots.
It contains 70 vol% of tetrasilicic fluormica crystals, approx. 2μm in
diameter.
The mechanical properties of Dicor MGC are similar to those of Dicor
glass-ceramic, although it has less translucency.
79.
Advantages
• Improved aesthetics
•Minimal processing shrinkage
• Good marginal fit
• Moderately high flexural strength
• Low thermal expansion equal to that of tooth structure
• Minimal abrasiveness to tooth enamel
Disadvantages
• Limited use in low stress areas
• Inability to be coloured internally
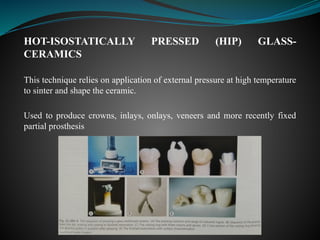
HOT-ISOSTATICALLY PRESSED (HIP)GLASS-
CERAMICS
This technique relies on application of external pressure at high temperature
to sinter and shape the ceramic.
Used to produce crowns, inlays, onlays, veneers and more recently fixed
partial prosthesis
82.
Advantages
• Translucent ceramiccore
• Moderately high flexural strength
• Excellent fit
• Excellent aesthetics
Disadvantages
• Potential to fracture in posterior areas
• Need to use a resin cement to bond the crown micromechanically to
tooth structure
Uses
• ICS- anteriorsingle unit inlays, onlays, crowns and veneers
• ICA- anterior and posterior crowns and anterior three-unit FPDs.
• ICZ- posterior crowns and posterior FPDs.
90.
Advantages
• Lack ofmetal
• Relatively high flexural strength and toughness
Disadvantages
• High degree of opacity
• Technique sensitive
• Long processing time
Advantages
• Negligible porositylevels
• Freedom from making an impression
• Reduced assistant time associated with impression procedures
• Single patient appointment (Cerec system)
• Good patient acceptance
Disadvantages
• Need for costly equipment
• Lack of computer controlled processing support for occlusal adjustment
• Technique sensitive
97.
• Anusavice, Shen,Rawls. Phillips’ Science of Dental Materials.
Elsevier.2013;12edi.
• Powers JM, Sakaguchi RL. Craig’s Restorative Dental Materials.
Elsevier.2006;13edi.
• Bonsor SJ, Pearson GJ. A clinical guide to applied dental materials.
Elsevier.2013.
• Rosenblum MA, Schulman A. A review of all-ceramic restorations.
JADA 1997;128(3):297-307.
REFERENCES
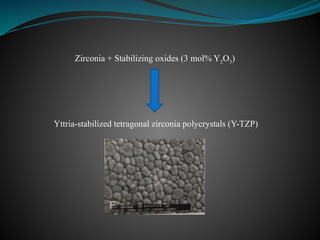
• Zirconium dioxide(ZrO2)or
zirconia, is a white crystalline
oxide of zirconium.
• Found as naturally occuring
mineral in igneous rock.
• The advent of zirconia (ZrO2) as a
high performing ceramic has its
origins in a classic paper by Garvie
et al(1975) and subsequent work of
others in the materials science
community(Green et al. 1989).
• Used in dentistry for crown and
bridge applications since 2004.
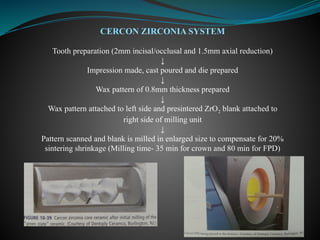
CERCON ZIRCONIA SYSTEM
Toothpreparation (2mm incisal/occlusal and 1.5mm axial reduction)
↓
Impression made, cast poured and die prepared
↓
Wax pattern of 0.8mm thickness prepared
↓
Wax pattern attached to left side and presintered ZrO2 blank attached to
right side of milling unit
↓
Pattern scanned and blank is milled in enlarged size to compensate for 20%
sintering shrinkage (Milling time- 35 min for crown and 80 min for FPD)
111.
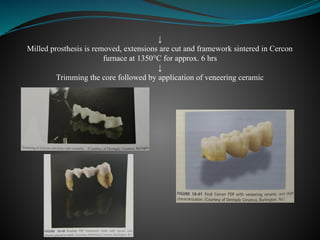
↓
Milled prosthesis isremoved, extensions are cut and framework sintered in Cercon
furnace at 1350°C for approx. 6 hrs
↓
Trimming the core followed by application of veneering ceramic
114.
• Anusavice. Phillips’Science of Dental Materials. Elsevier.2010;11edi.
• Anusavice, Shen, Rawls. Phillips’ Science of Dental Materials.
Elsevier.2013;12edi.
• Powers JM, Sakaguchi RL. Craig’s Restorative Dental Materials.
Elsevier.2006;13edi.
• Bonsor SJ, Pearson GJ. A clinical guide to applied dental materials.
Elsevier.2013.
• Zhang Y, Lawn BR. Novel Zirconia materials in Dentistry. Journal of Dental
Research 2018;97(2):140–147.
REFERENCES


































































![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)








![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)






