

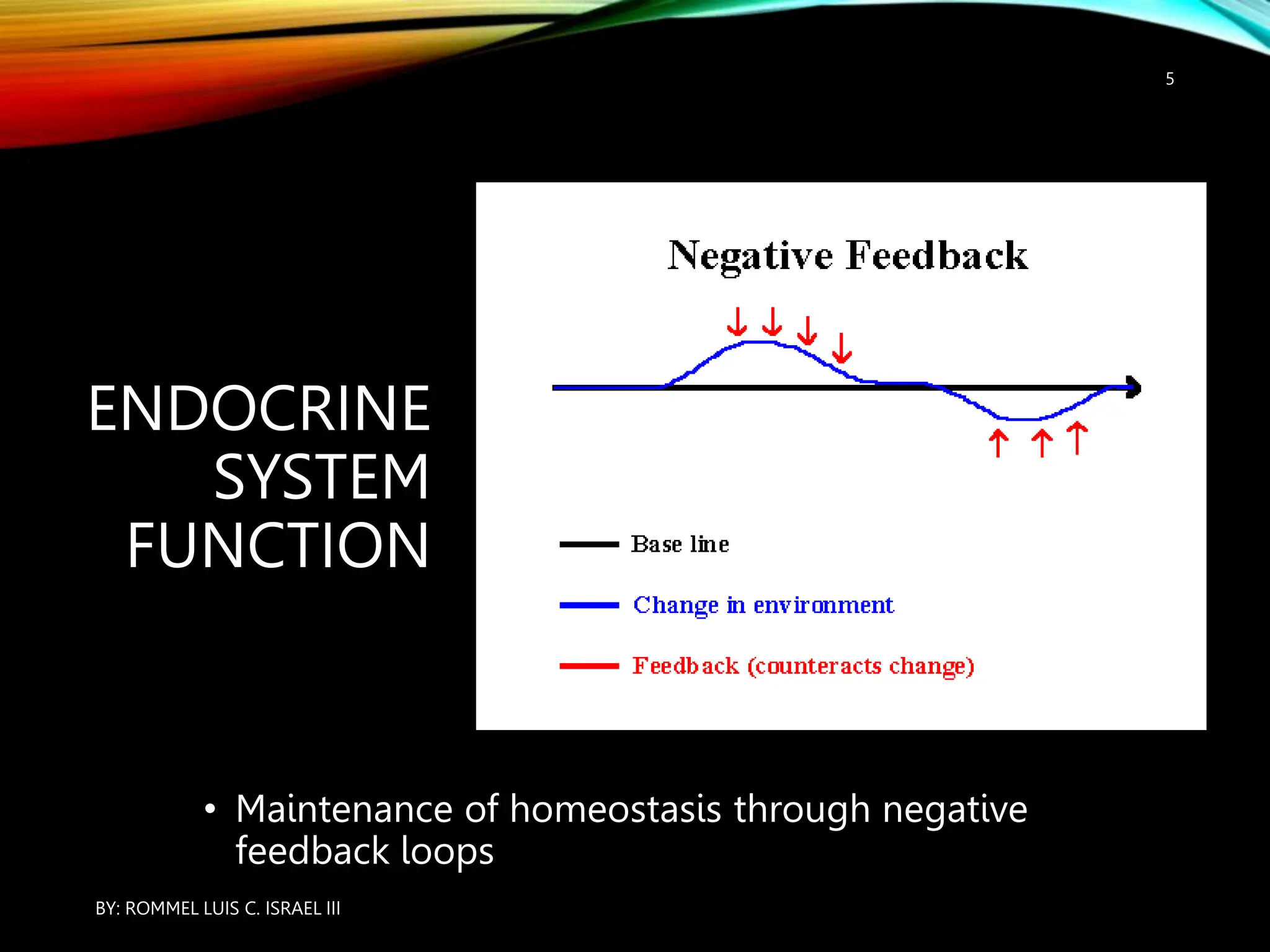

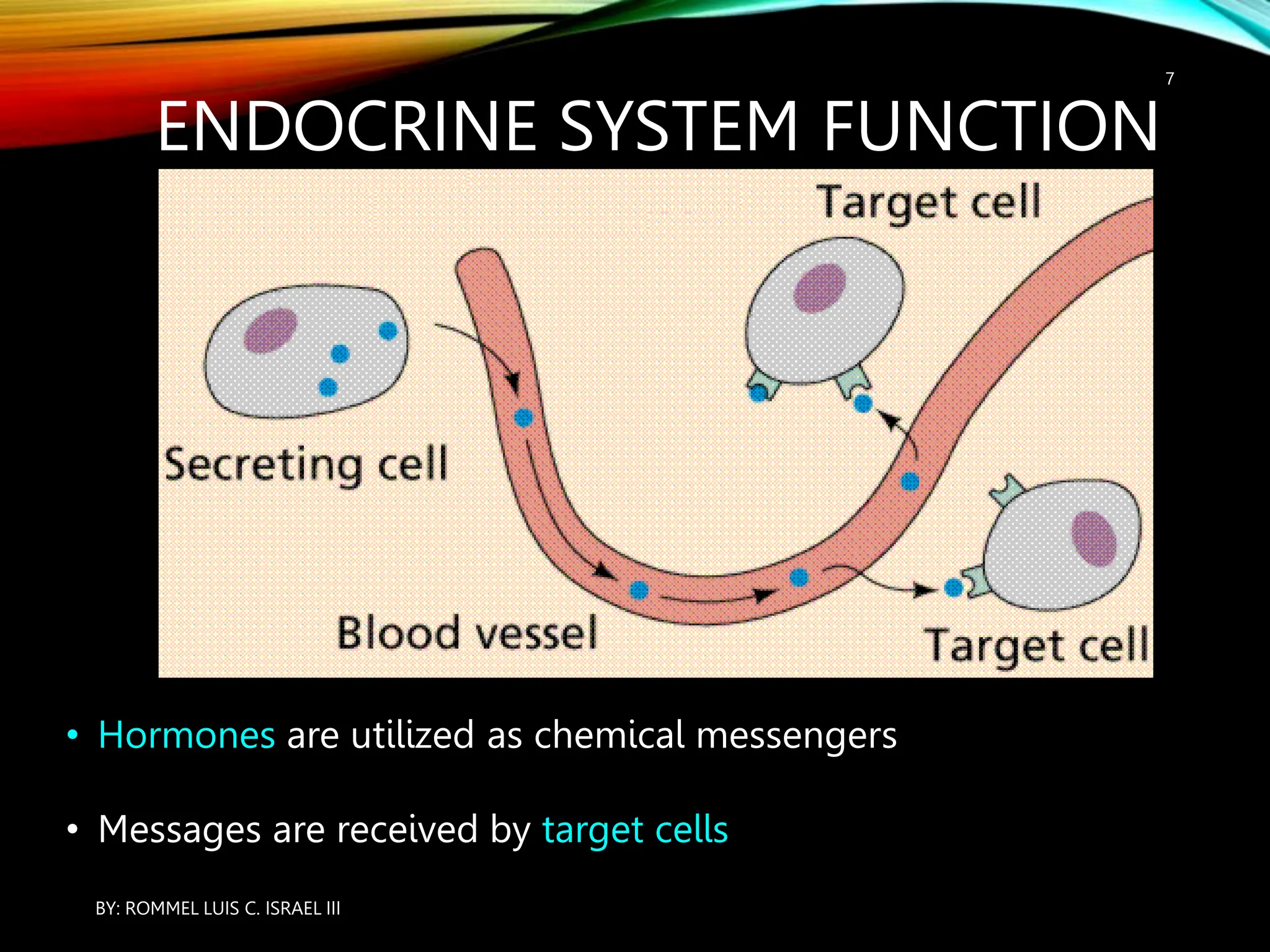










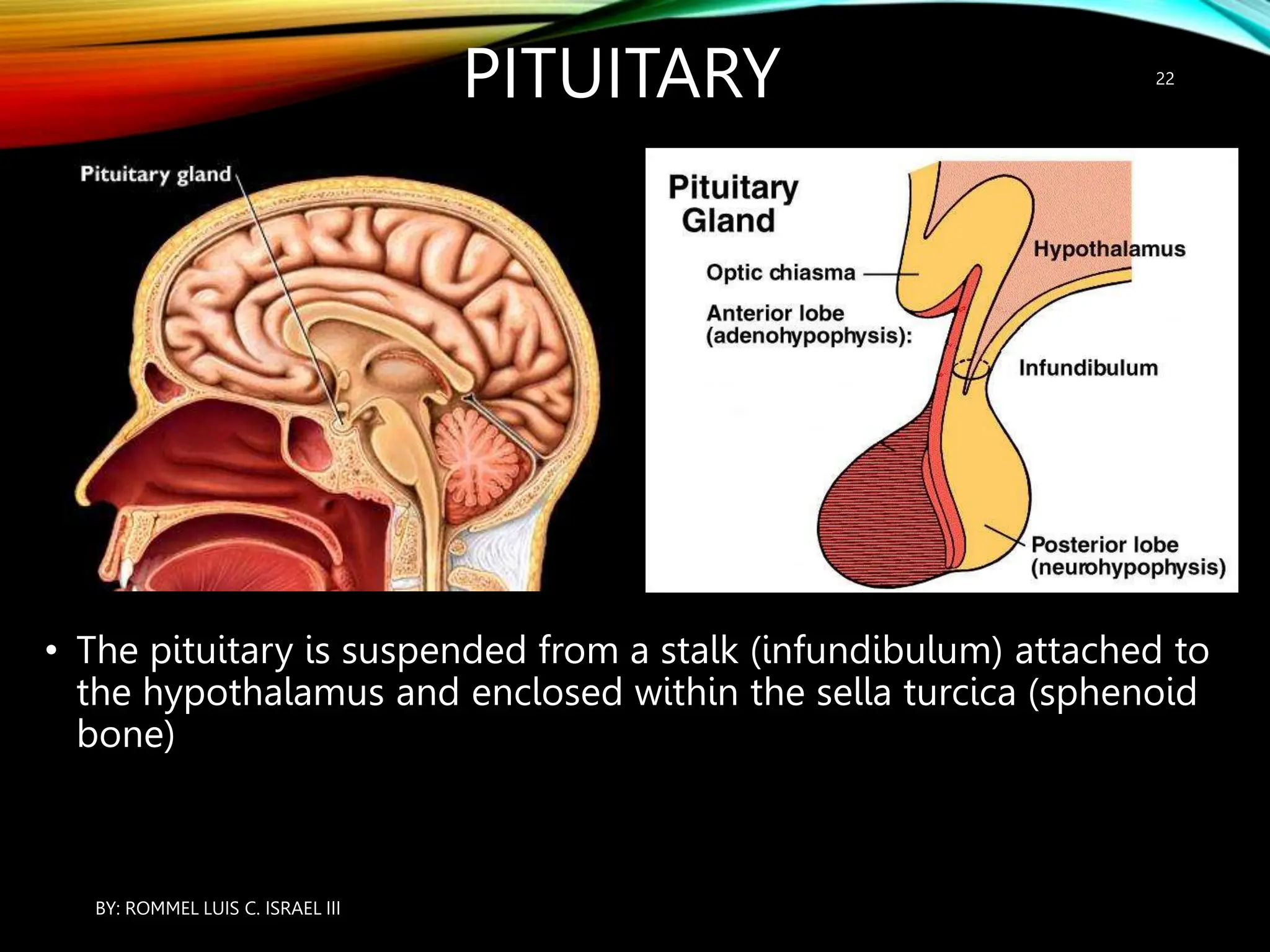





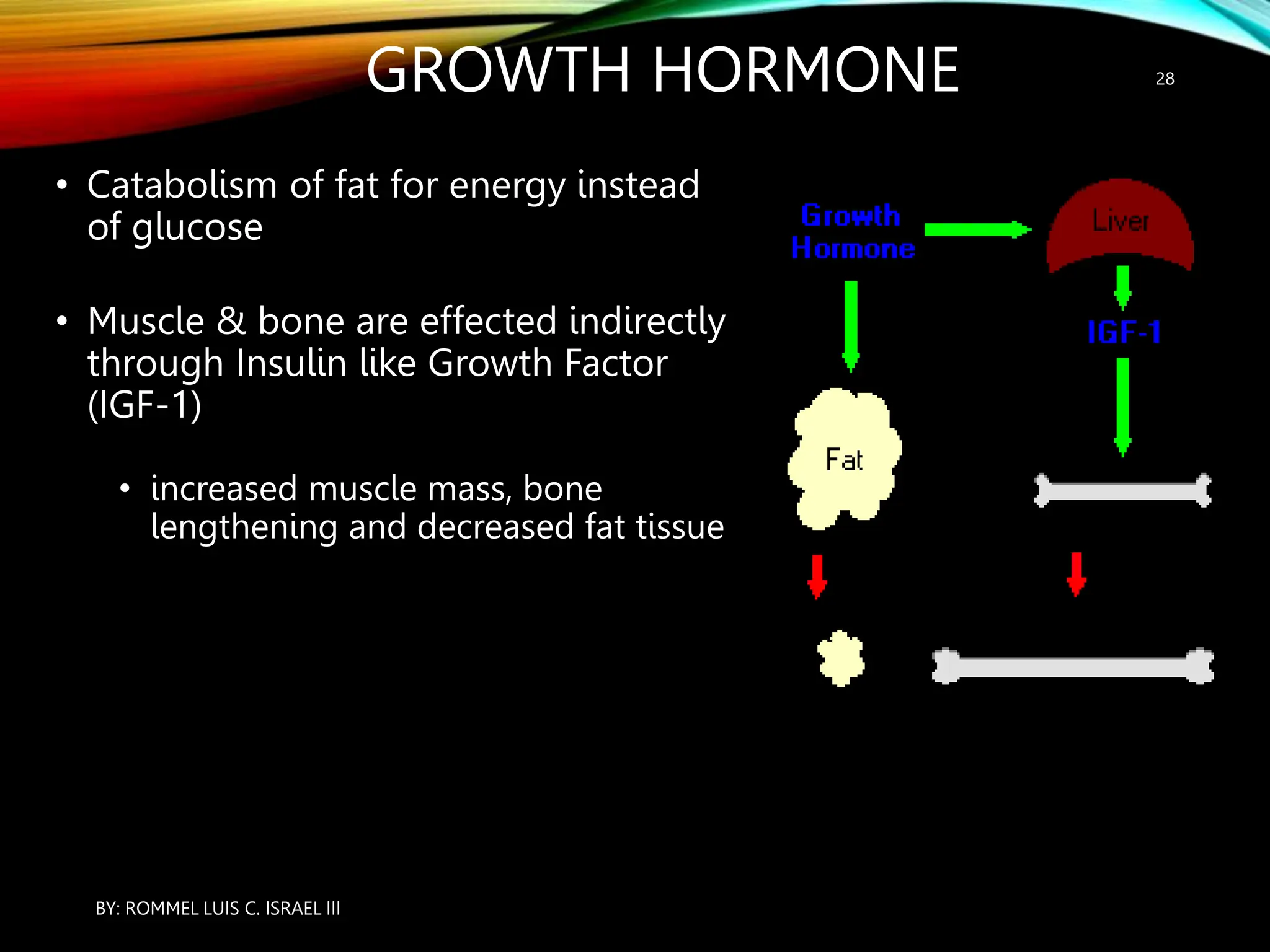

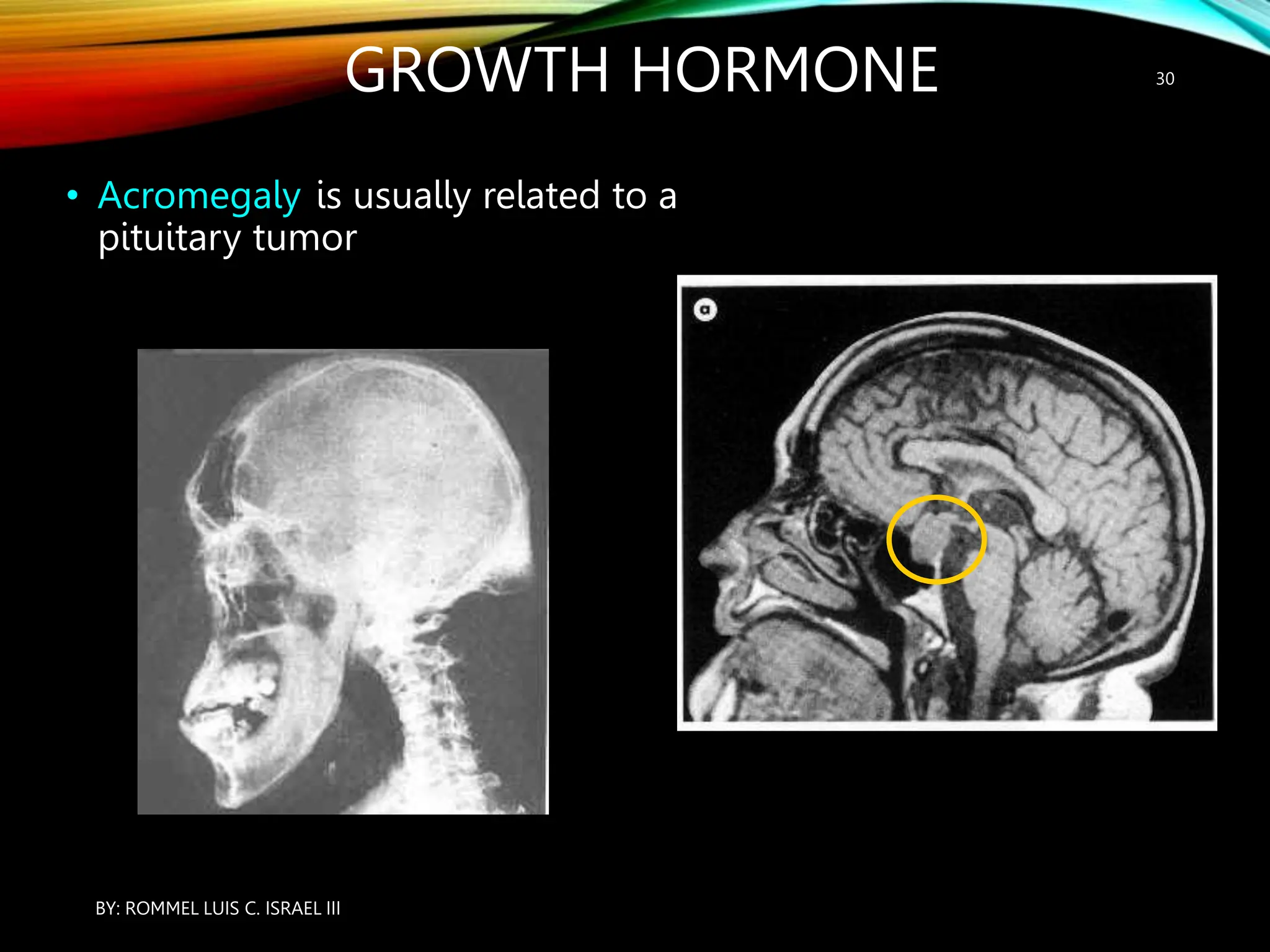


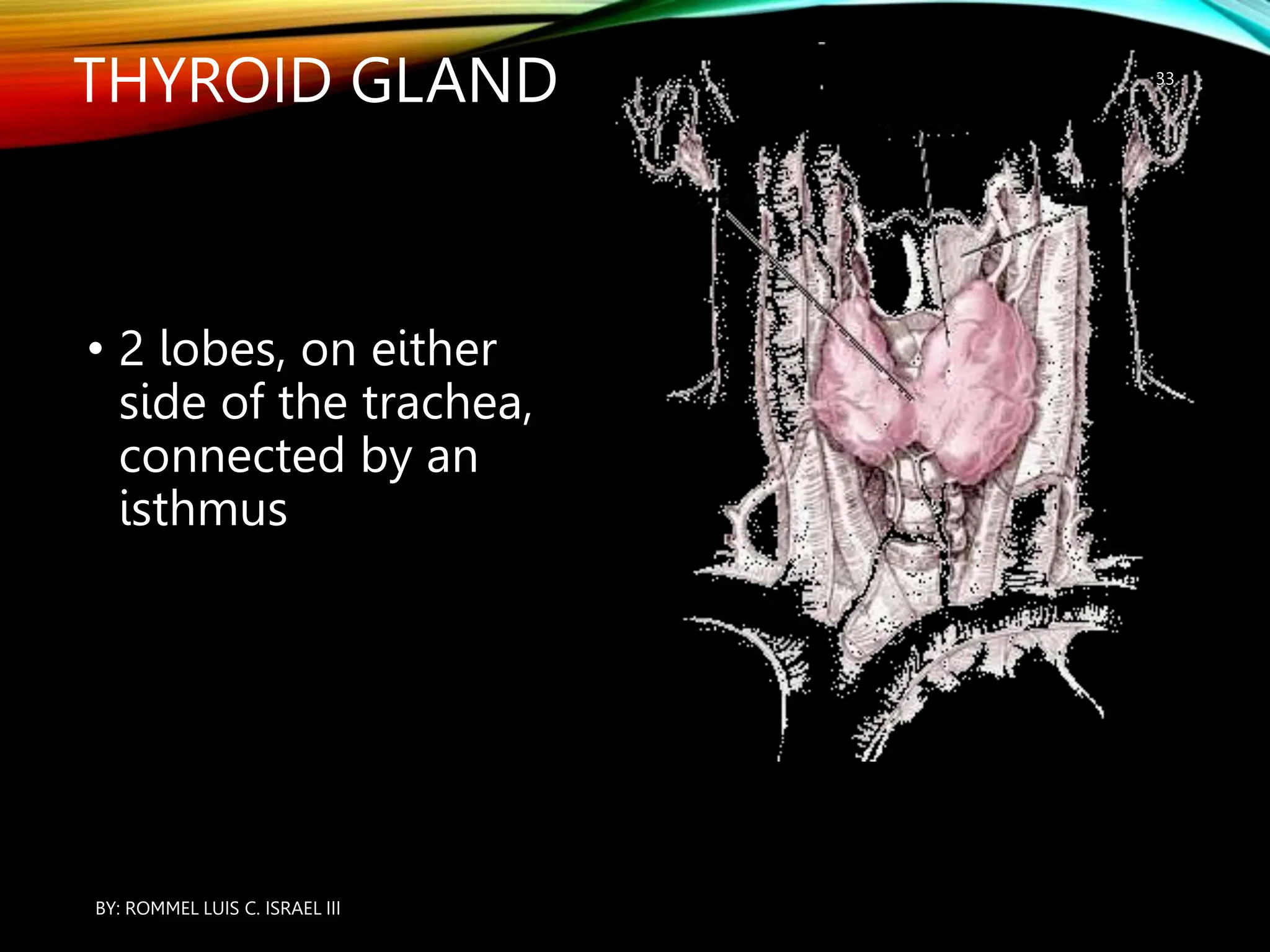

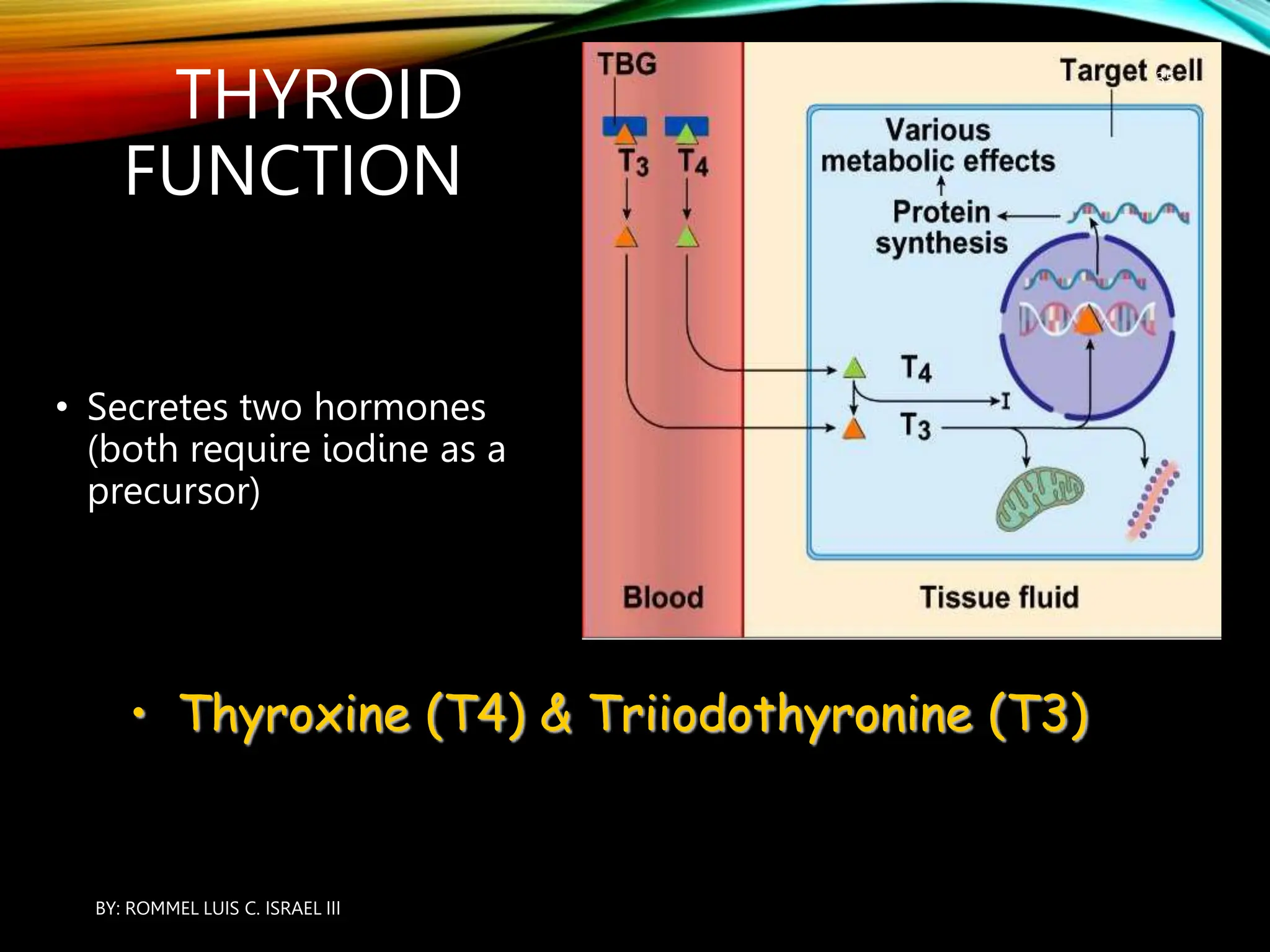




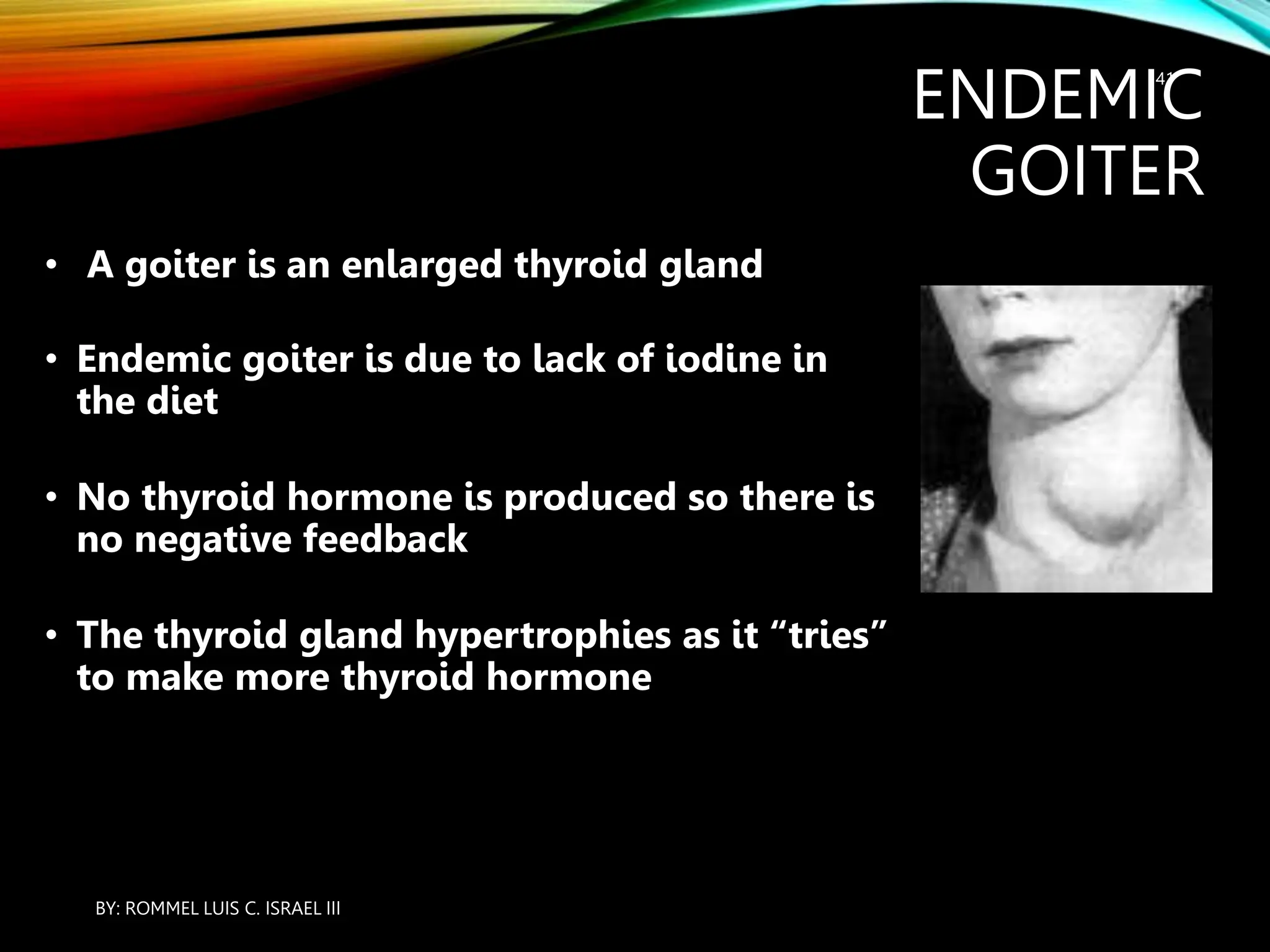

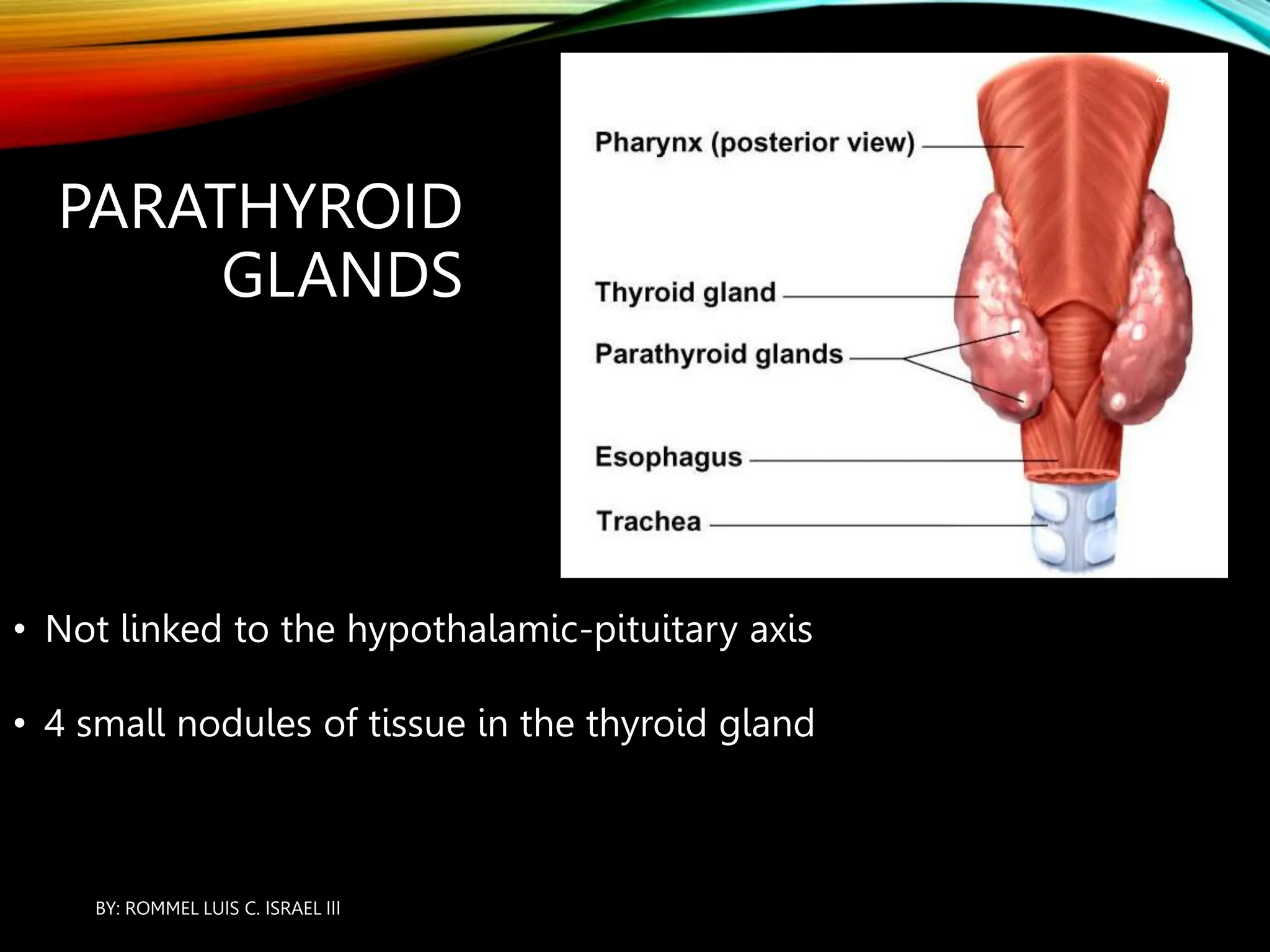








































The document provides an overview of the endocrine system, including its major glands and hormones. It discusses the classical endocrine glands like the pituitary, thyroid, and adrenals. It explains how the hypothalamus regulates the pituitary which in turn regulates other glands. The pituitary is divided into the anterior and posterior portions. Hormones communicate between organs through negative feedback loops or by binding to target cells. The functions and mechanisms of several key hormones are reviewed like growth hormone, thyroid hormones, and parathyroid hormone.























































































