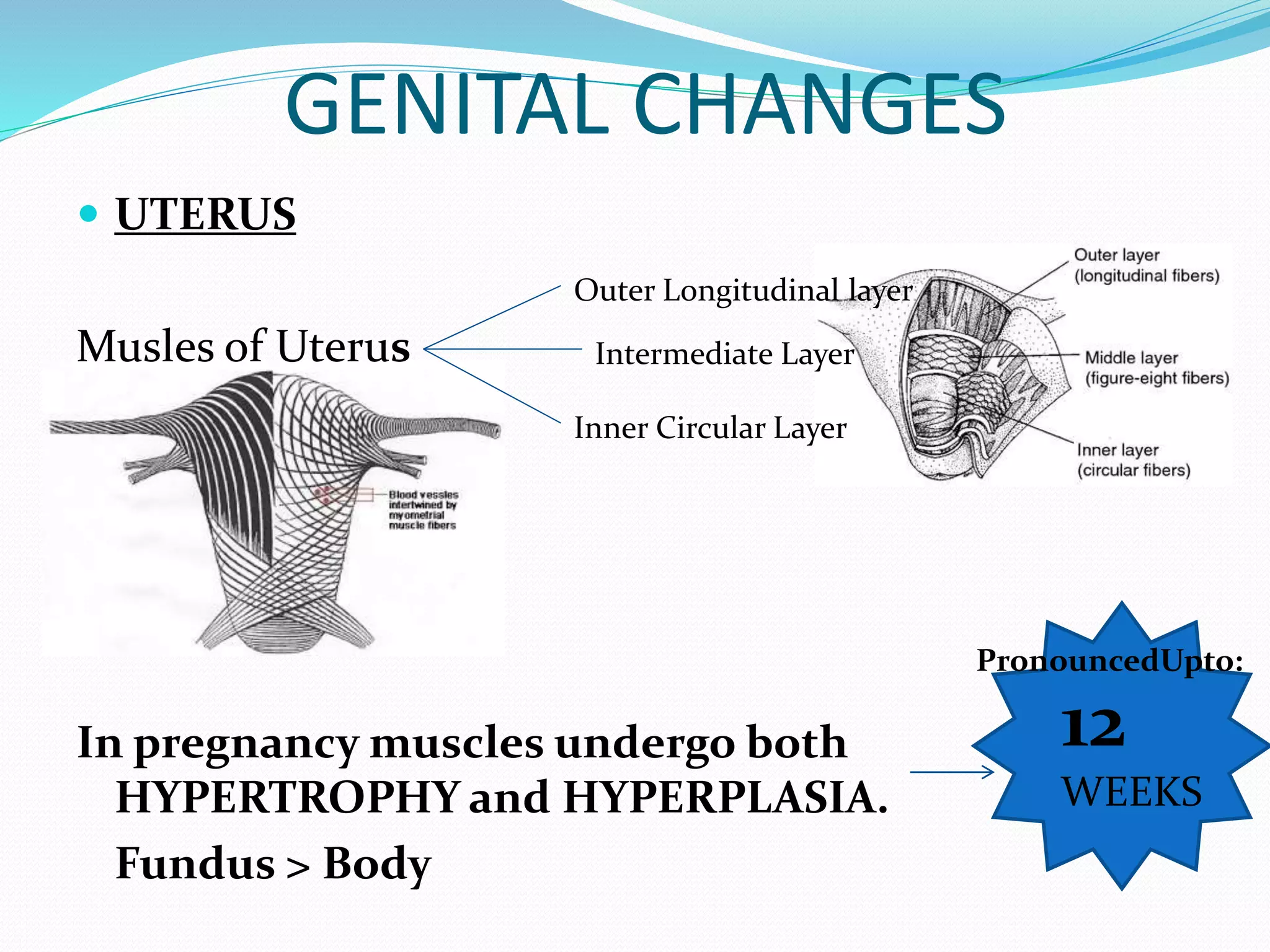
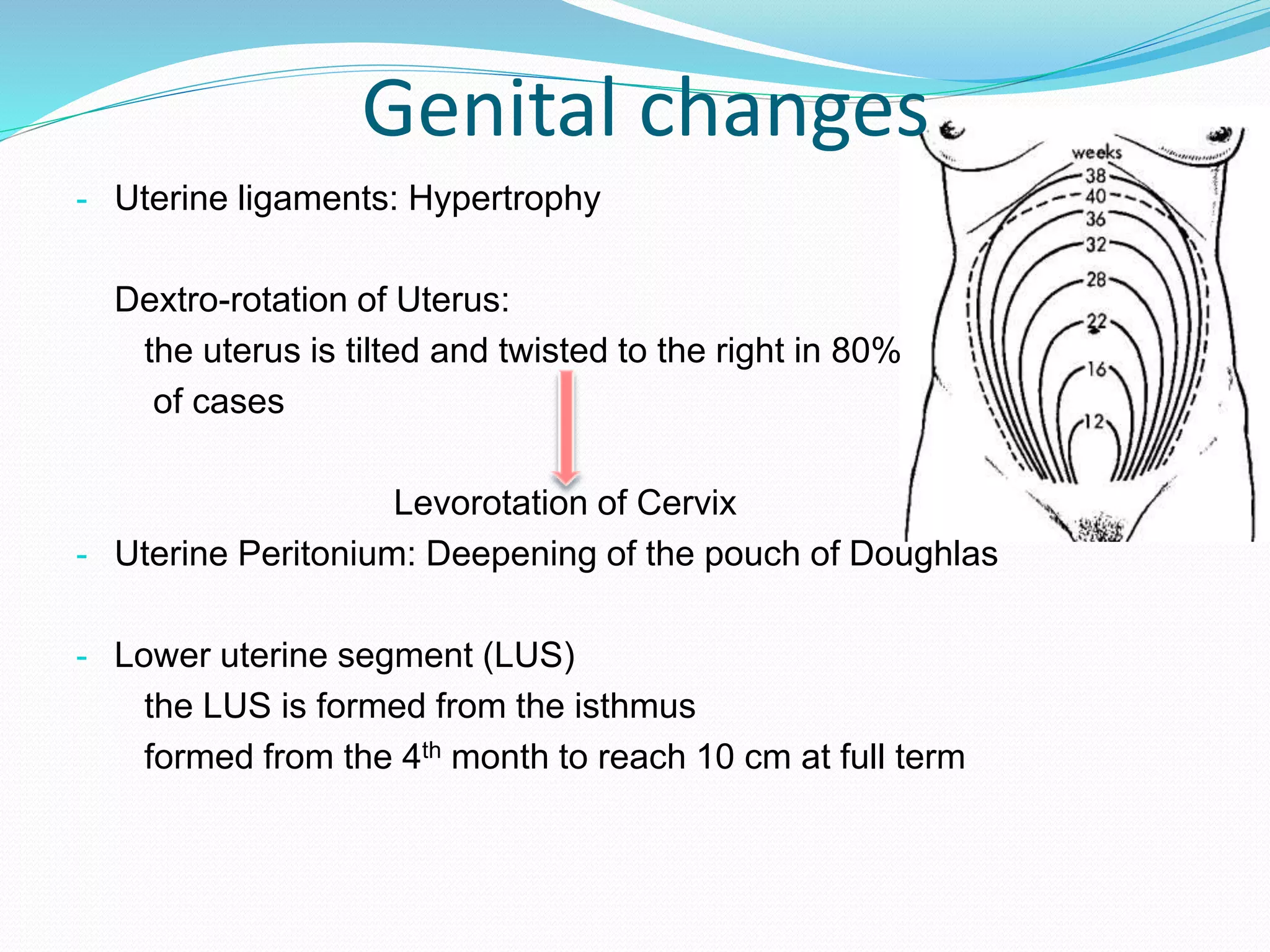
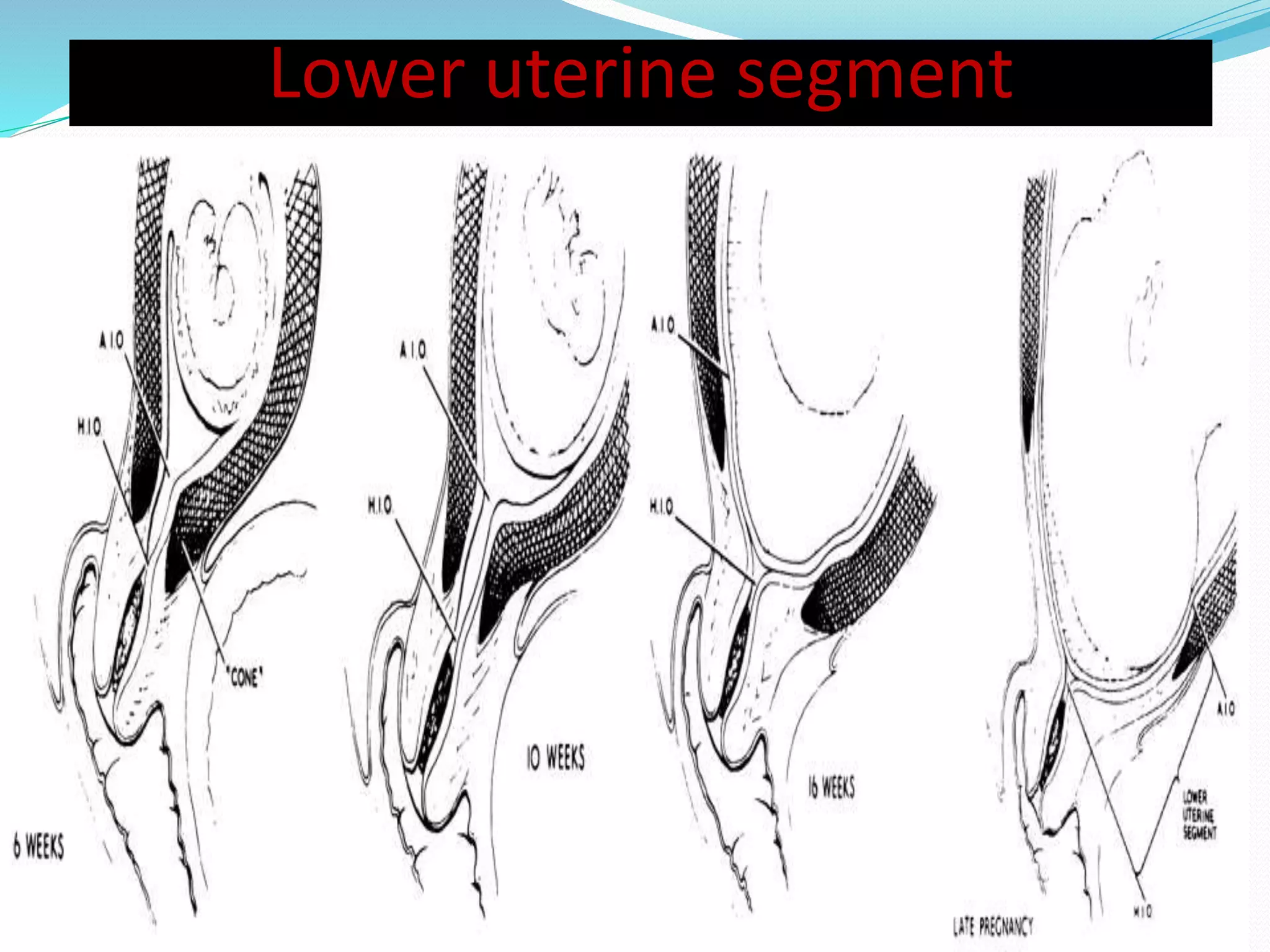
The document summarizes various anatomical, physiological, and biochemical changes that occur during pregnancy across multiple body systems. Key anatomical changes include uterine enlargement, breast changes, skin changes like lineae nigra and striae gravidarum. Physiological changes impact the cardiovascular, respiratory, renal and endocrine systems to support the nutritional and oxygen needs of the growing fetus. Hematological changes include increased blood volume and mild anemia. Biochemical changes involve iron metabolism and increased production of hormones like estrogen, progesterone, human placental lactogen and relaxin.