Physiological changes during pregnancy can be extensive. The document summarizes several key changes:
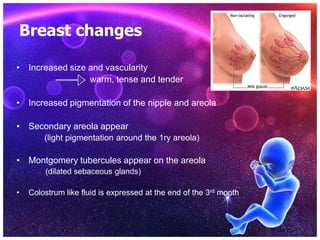
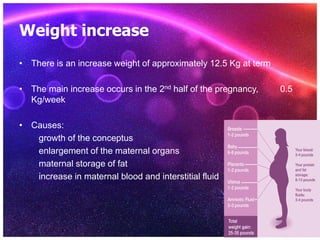
1) The uterus grows enormously in size and weight to accommodate the growing fetus. Other genital organs like the cervix and breasts also see significant changes to support pregnancy and birth.
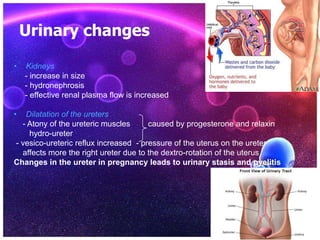
2) Extensive changes occur in many body systems like the cardiovascular, respiratory, urinary and endocrine systems to support the nutritional and oxygen needs of the mother and fetus. This includes increases in blood volume, cardiac output, kidney size and lung capacity.
3) Hormonal changes are also profound, with high levels of progesterone, estrogen and other placental hormones influencing many processes and organs across the body to sustain the pregnancy.