Downloaded 49 times

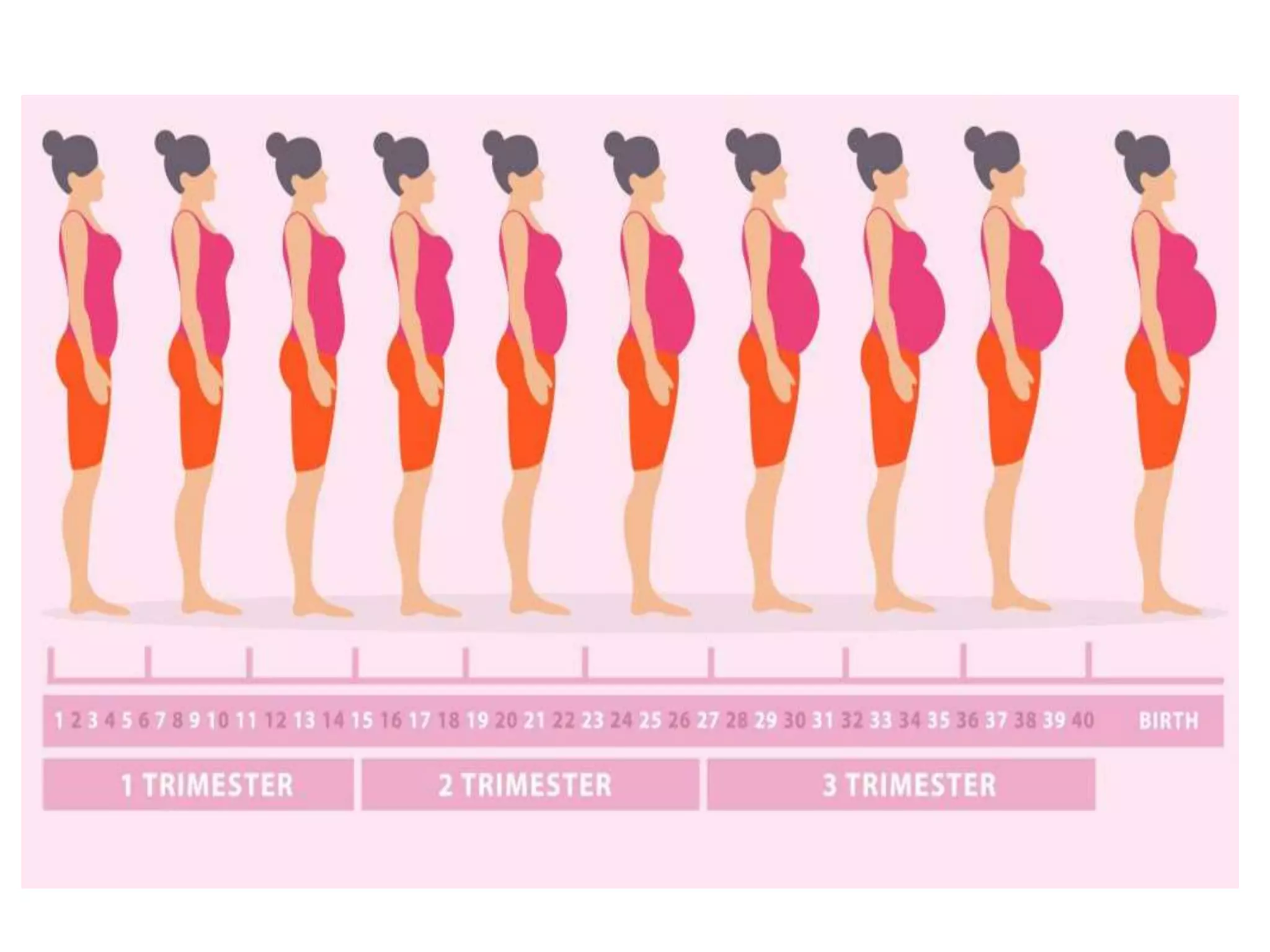

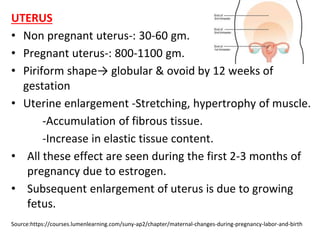

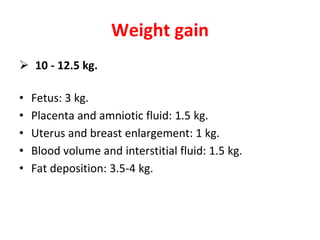



The document summarizes several physiological changes that occur during pregnancy. The uterus enlarges significantly from 30-60 grams to 800-1100 grams due to stretching, hypertrophy, increased tissue, and accumulation of fibrous tissue stimulated by estrogen. The cervix and vagina undergo changes like increased vascularity and thickness. Other systems affected include increased blood volume, cardiovascular changes like lower blood pressure, respiratory changes like increased ventilation, and renal changes like increased glomerular filtration rate. Hormonal changes induce thyroid and adrenal gland enlargement along with increased secretions. Psychological changes can include mood alterations and sleep decreases. The document also briefly outlines metabolic changes like increased weight gain and retention of water and sodium. Pregnancy tests







































![Physiological and psychological changes during pregnancyhanges [Recovered].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/ppchangesrecovered-240119155912-065d14b8-thumbnail.jpg?width=640&height=640&fit=bounds)















































