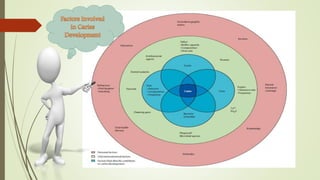
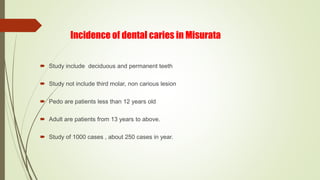
Dental caries is an irreversible disease characterized by the demineralization and destruction of tooth tissues, resulting in various classifications based on anatomic site, extent, and progression. The document discusses different types of dental caries, including pit and fissure caries, smooth surface caries, and various forms based on progression like acute, chronic, and nursing bottle caries. It also examines diagnostic methods, histopathology, contributing factors, and research findings from studies conducted in Misurata on the incidence of dental caries.