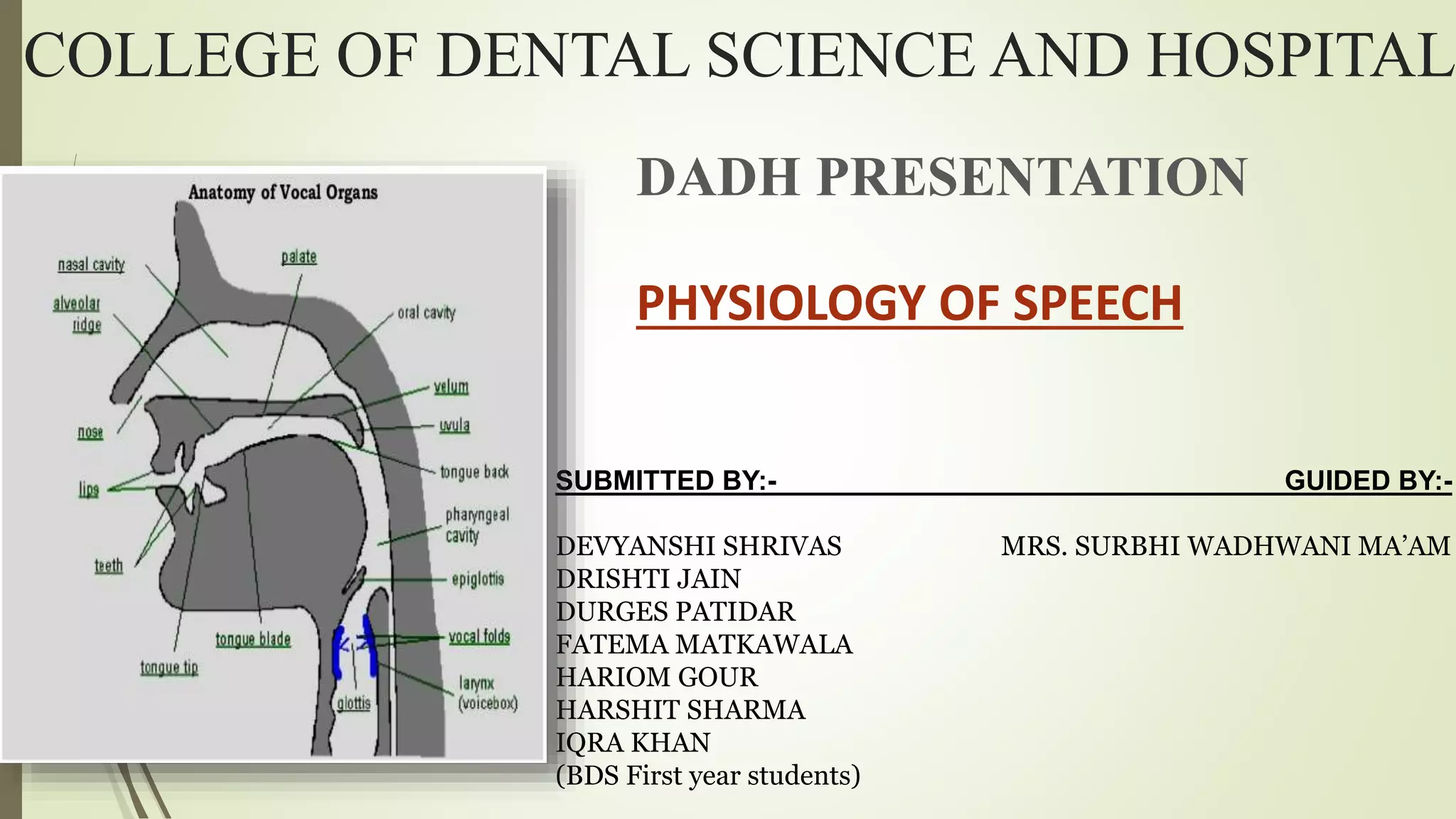


































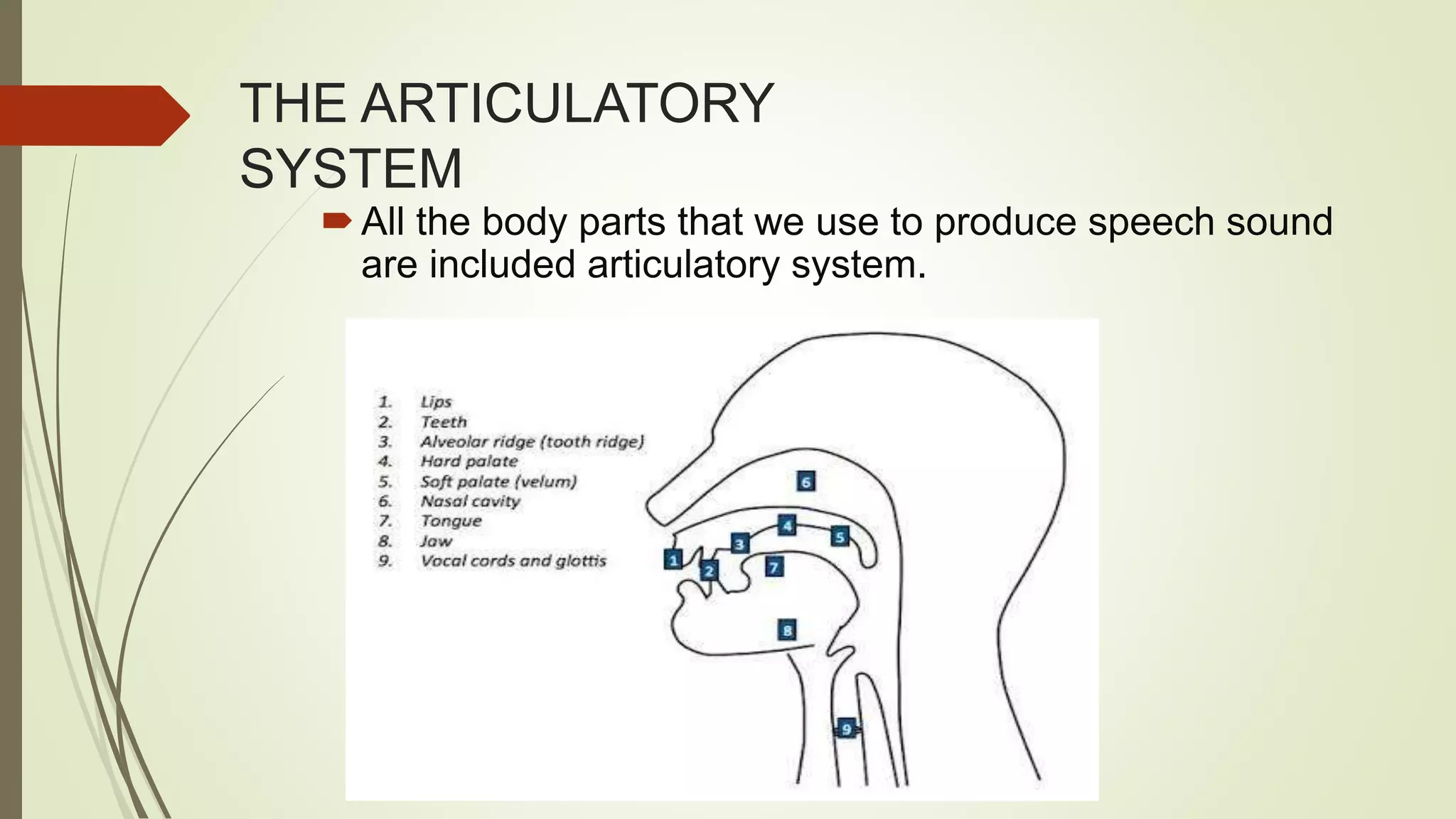
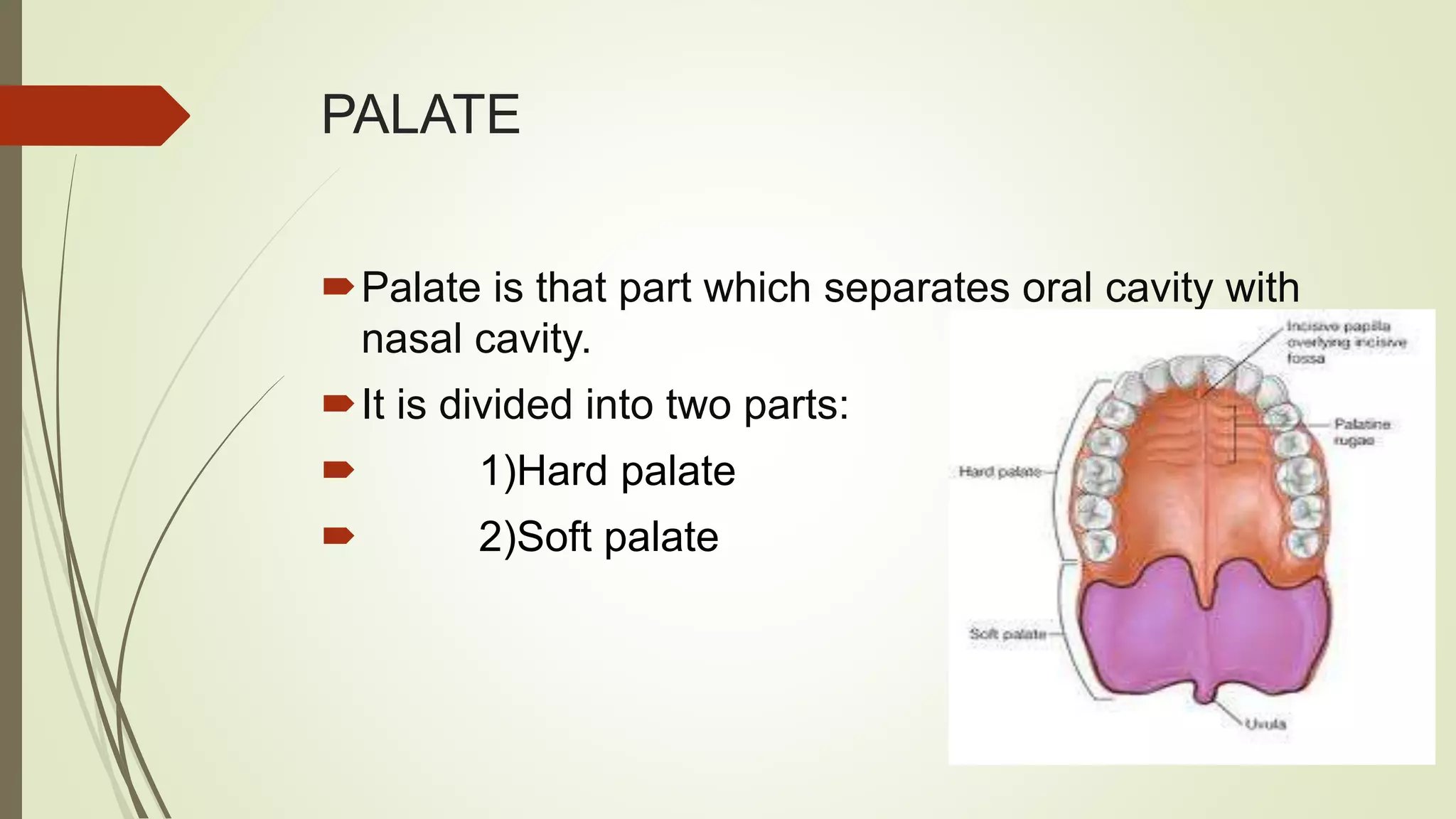




























This document provides an overview of the anatomy and physiology of speech. It begins with the basic anatomy of the larynx and vocal cords. It then discusses the anatomy of the larynx in more detail, including its location, size, constituent cartilages and cavities. It describes the intrinsic and extrinsic laryngeal muscles. It explains the movements of the vocal folds and their role in voice production. It discusses the stages of voice production including compression, vibration, amplification and modification. It covers respiration, phonation and resonance. It also discusses the role of the palate, teeth and tongue in voice production and defines what a speech prosthesis is.



































































