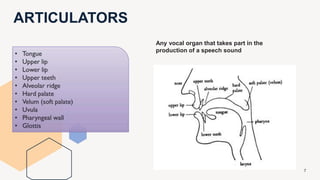
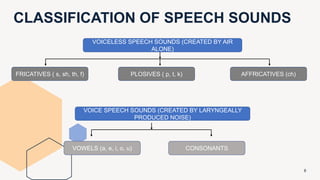
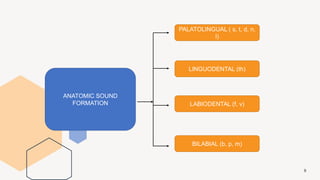
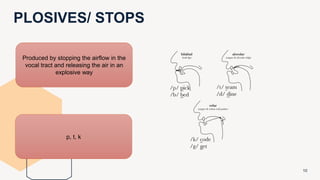
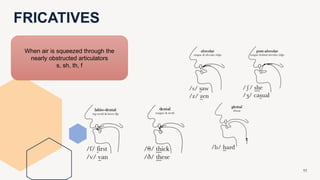
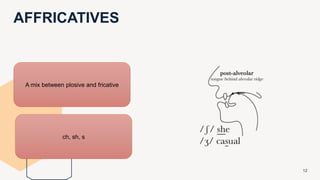
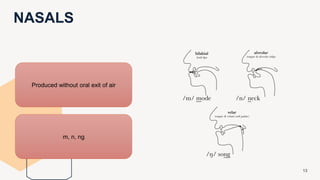
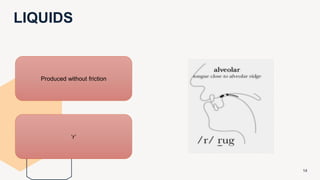
This document discusses phonetics and speech production as it relates to prosthodontic considerations. It covers topics such as the classification of speech sounds, methods of speech analysis, and how to position teeth during denture fabrication to facilitate proper speech. The production of specific sounds like 's' and 'f' are examined in detail. The document emphasizes that the dentist should understand speech mechanics to avoid creating speech difficulties when providing dental treatments like complete dentures.