Downloaded 19 times
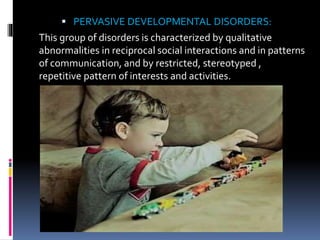
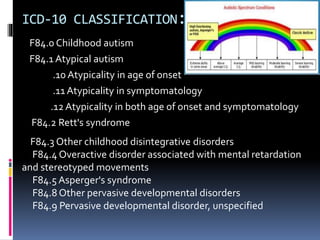
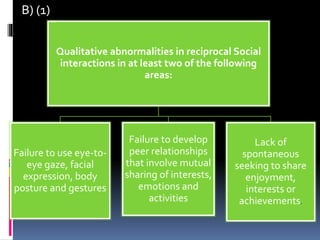
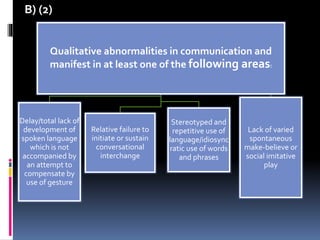
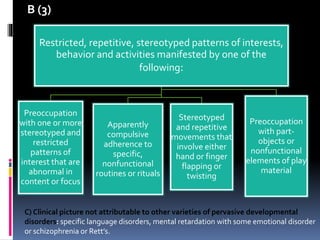

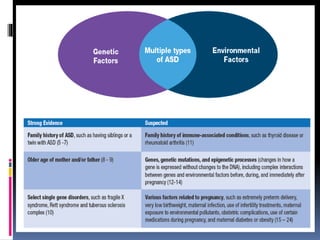





The document provides an overview of pervasive developmental disorders, including their classifications, diagnostic guidelines, and management strategies. It discusses specific conditions such as autism, Asperger's syndrome, and Rett's syndrome, outlining their characteristics, symptoms, and approaches to treatment. Additionally, it highlights the importance of early intervention and tailored educational and therapeutic practices to support individuals affected by these disorders.









































![Odu%20 clinical%20science%20iii%20pdd%202011[1]](https://cdn.slidesharecdn.com/ss_thumbnails/odu20clinical20science20iii20pdd2020111-111213211620-phpapp02-thumbnail.jpg?width=640&height=640&fit=bounds)

























