Downloaded 117 times
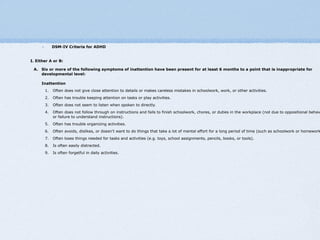
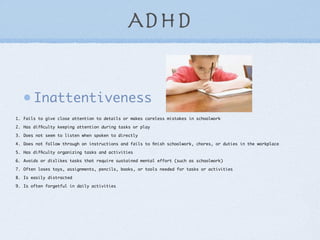
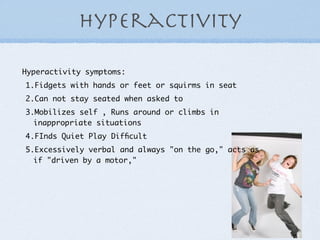




ADHD is a common disorder affecting 3-5% of school-aged children. It is characterized by inattentiveness, hyperactivity, and impulsivity. Diagnosis involves evaluating symptoms, which must be present in multiple settings, and determining impairment. Treatment may include behavioral therapy, environmental modifications, medications like stimulants, and an IEP. Nurses play an important role in medication administration, safety, behavioral observation, advocacy, and supporting adherence to treatment plans.
































![ADHD (best)]](https://cdn.slidesharecdn.com/ss_thumbnails/bykhaihojoshuagabriel1-1234763718979961-1-thumbnail.jpg?width=640&height=640&fit=bounds)

























