Peripheral nerve biopsy
•Download as PPTX, PDF•
5 likes•1,669 views

This document discusses nerve biopsy interpretation. It begins by describing nerve anatomy and indications for biopsy such as vasculitis and neuropathy. The sural nerve is preferred for biopsy due to its sensory function and distal location. Processing involves formalin, glutaraldehyde and cryosectioning. Stains identify morphology, myelin, and amyloid. Features to examine include vasculature, demyelination, regeneration, and inflammation. Common neuropathies discussed are diabetic, inflammatory, leprosy, vasculitic and amyloid. Biopsy can reveal axonal damage or demyelination.

Recommended
More Related Content
What's hot
What's hot (20)
Similar to Peripheral nerve biopsy
Similar to Peripheral nerve biopsy (20)
More from Dr Sayan Das
More from Dr Sayan Das (15)
Recently uploaded
Recently uploaded (20)
Peripheral nerve biopsy
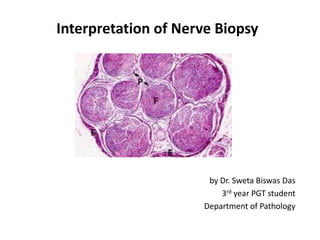
- 1. Interpretation of Nerve Biopsy by Dr. Sweta Biswas Das 3rd year PGT student Department of Pathology
- 2. INTRODUCTION Each peripheral nerve composed of one or more bundles (fascicles) Each nerve fibre surrounded by loose vascular supporting tissue endoneurium Each fascicle surrounded by condensed collagenous tissue perineurium All fascicles are surrounded by loose collagenous tissue epineurium
- 3. Peripheral nerve in transverse section
- 4. INDICATION FOR NERVE BIOPSY Vasculitic Neuropathy Neuropathy Associated With Infection Inflammatory Demyelinating Polyneuropathy Sarcoid Neuropathy Amyloid Neuropathy Diabetic Neuropathy Toxic induced neuropathy
- 5. SELECTING THE NERVE FOR BIOPSY Distal lower limbs –Sural nerve or superficial peroneal nerve Upper limbs-Superficial radial nerve or a branch of ulnar nerve Progressive optic neuropathy-Optic nerve biopsy
- 6. SURAL NERVE BIOPSY Easily identifiable . Purely sensory – No motor deficit occur following biopsy. Liable to be affected by neuropathy distal branch of a long nerve.
- 7. PROCESSING OF NERVE BIOPSY 1.5 2 1.5 5 cm Neutral-buffered formalin 4 % Glutaraldehyde -180°C liquid Nitrogen Paraffin section Semithin section Thin section for EM Frozen section H&E Modified trichrome Congo red Toluidine blue Toluidine blue and basic fuchsin H&E Modified trichrome Congo red Cresyl-fast-violet
- 8. Advantages and Disadvantages of tissue Sections Frozen section Rapid diagnosis Immunofluorescent studies Relative ease for preserving the longitudinal section for segmental demyelination Detail of the cells are not clear Paraffin section Details of cell and anatomical structure Artifact is unavoidable Semithin section Detection thinly myelinated fibers Detection of onion bulb Detection clustering of regenerated fibers Special training EM section The only test for the unmyelineated fibers Special training
- 9. STANING Different stains Staining for H&E Morphology, Vasculitis, Inflammation, Myelin ovoids, axonal degeneration Masson's Trichrome Fibrosis, Hyalinisation,Vessels Luxol fast blue Myelin Toluidine Myelin Congo red Amyloid IHC EMA ,S100,MBP,PMP22
- 10. H&E Stain of peripheral nerve
- 11. Toluidine blue Stain of peripheral nerve
- 12. TRICHROME STAIN
- 13. WHAT TO LOOK FOR Status of the epineurium including the blood vessels Alterations in the perineurium Endoneurium oedema Density of the large and small myelinated nerve fibers Extent of axonal degeneration and atrophy Frequency of bands of Bungner and Myelin degeneration Number of macrophages cluster Onion bulb formation Inflammatory infiltrates Presence/absence of amyloid
- 14. Wallerian degeneration Degeneration of axon distally following its interruption Distal to injury the axon disintegrates and the myelin breaks up into globules Macrophages participate in the removal of axonal and myelin debris Approximation of nerve ends result in regeneration, the basement membrane of the schwann cell survives and acts as skeleton along which the axon regrows
- 15. SEGMENTAL DEMYELINATION Scattered destruction of the myelin sheath occurs without axonal damage The primary lesion affects the schwann cell. Prognosis for recovery is good because the muscle is not denervated
- 17. ONION BULB FORMATION Refers to the concentric laminated layers surrounding the nerve fibre. Best detected in the semithin section Pathogenetically , onion bulb formation is indication of repeated demyelination and remyelination
- 19. INFLAMMATORY DEMYELINATING POLYNEUROPATHY Acute- Guillain Barré Syndrome Acute onset immune mediated demyelinating neuropathy Weakness beginning in the distal limbs and rapidly advances to affect proximal muscle function(ascending paralysis) Prior history of viral infection Hallmark of inflammatory neuropathy- presence of inflammatory cells in the endoneural space of the nerve Inflammatory cells are primarily responsible for the macrophage induced demyelination in these neuropathy
- 20. Chronic inflammatory Demyelinating Poly radiculoneuropathy Symmetrical mixed sensorimotor polyneuropathy that persists for more than 2 months Evidence of recurrent demyelination and remyelination associated with proliferation of Schwann cells ,formation of onion bulbs INFLAMMATORY DEMYELINATING POLYNEUROPATHY
- 21. ONION BULB
- 22. LEPROSY M. leprae is the bacterium that invades peripheral nerve Common nerves are Ulnar nerve at the elbow Deep peroneal branch at the ankle
- 23. TUBERCULOID LEPROSY Pathological hallmark is an intense inflammatory granulomatous lesion that severely damages the neural architecture Axon ,schwann cells and myelin lost Granulomas in the epineural and perineural spaces & edoneural space. Bacilli are scanty , Localized nerve involvement Healing –fibrosis and hyalization in the endoneurium and thick perineurial and epineurial sheaths
- 25. LEPROMATOUS LEPROSY Perineural and endoneural infiltration of enlarged macrophages and Schwann cells with M leprae bacilli and inflammatory cells. In severe cases the epineurium may be infiltrated by huge numbers of foamy cells especially around blood vessels. Granulomatous inflammatory response minimal. Segmental demyelination and remyelination and loss of both myelinated and unmyelinated axon Symmetric polyneuropathy
- 27. DIABETIC NEUROPATHY Ascending distal symmetric sensorimotor polyneuropathy Patients may be both type 1 and type 2 Nerve biopsy show reduced numbers of axons, degenerating myelin sheaths and regenerative axonal clusters, Endoneurial arterioles show thickening ,hyalinization
- 28. Pathophysiology
- 30. VASCULITIC NEUROPATHY Predominantly axonal damage Perivascular inflammation with active or chronic vessel damage Patchy /multifocal nerve fibre loss hemosiderine deposits
- 32. SARCOID NEUROPATHY Noncaseating granuloma in the epineurium Axonal degeneration Numerous myelin ovoids
- 33. AMYLOID NEUROPATHY Neuropathies are usually distally accentuated and symmetrical, and multiple mono neuropathies may occur Predominantly of axonal type Amyloid may be deposited within endoneurium ,and epineurial vasculature Stain-Congo red and Thioflavin S or T
- 35. TOXIC NEUROPATHIES Heavy metals( lead , mercury, arsenic, thallium) Drugs Interfere Axonal transport ,axonal degeneration,
- 36. CLASSIFICATION OF TWO MAIN CATEGORIES AXONAL DEGENERATION VASCULITIC DIABETIC TOXIC AMYLOID SARCOID DEMYELINATION GBS CIDP
- 37. REFERENCES Robbins & Cotran Pathologic basic of disease Wheaters funtional histology The Washington Manual Of Surgical Pathology
- 38. THANK YOU