Download to read offline
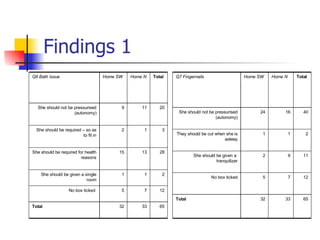
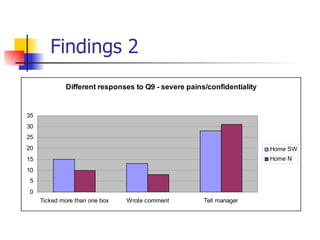
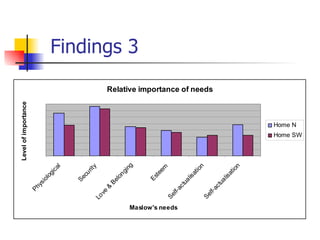
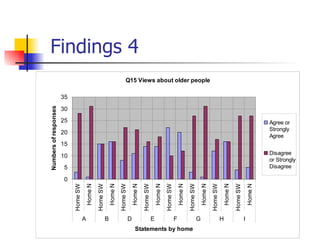
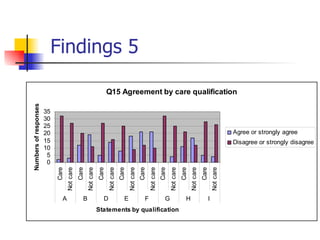
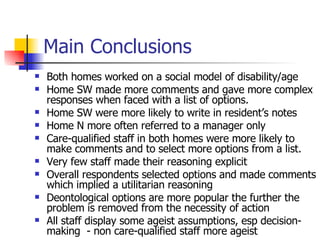
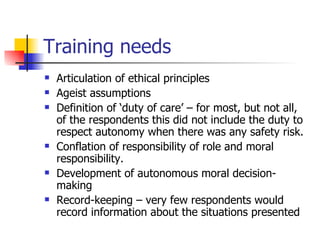

The document summarizes research conducted in two care homes that examined the values of different staff members in their work with older people. A questionnaire was administered to staff from various disciplines to analyze their responses to ethical dilemmas. The findings showed some differences between health and social care staff in their answers, though numbers were small. Overall, respondents displayed some ageist assumptions and a utilitarian approach to decision making. Training needs identified included articulating ethical principles, addressing ageist attitudes, defining duty of care, and developing autonomous moral decision making. The implications for service users were left for discussion.


























































































![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)


