1. A 20-year-old male was stabbed in the abdomen with a 10 cm knife during a fight. He was hemodynamically stable on arrival to the emergency room.
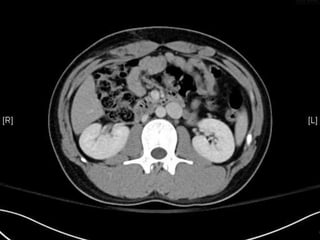
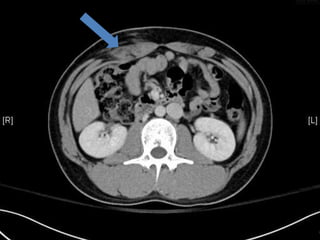
2. The emergency physician attempted to examine the wound but could not determine if it penetrated the peritoneum due to its depth. A CT scan or FAST exam was recommended to check for internal bleeding before deciding on observation or surgery.
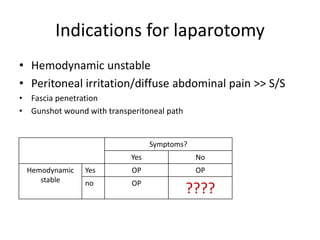
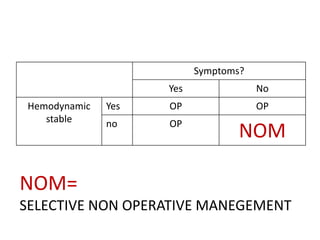
3. For hemodynamically stable patients with abdominal stab wounds, selective non-operative management is usually recommended initially. Further examination with CT scan is important to identify any internal bleeding before deciding on observation versus laparotomy.









































































![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)







![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)






