This document provides an overview of pelvis ring fractures, including:
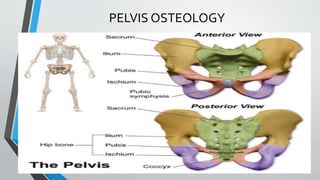
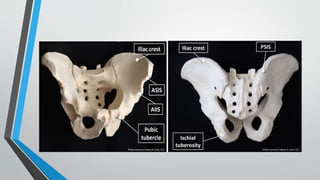
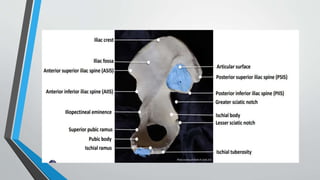
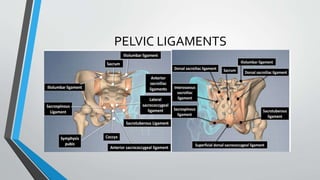
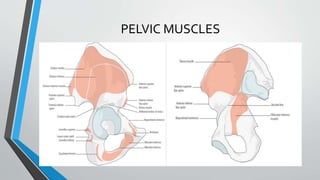
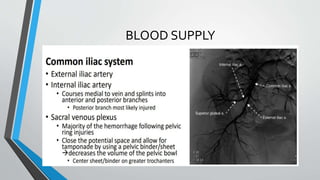
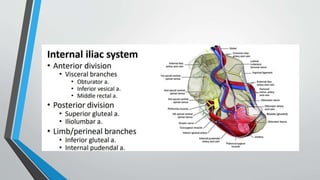
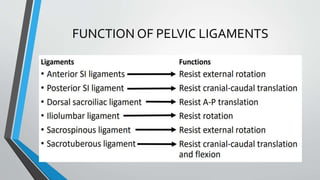
- The anatomy and blood supply of the pelvis.
- Common causes include motor vehicle accidents, falls, and osteoporosis.
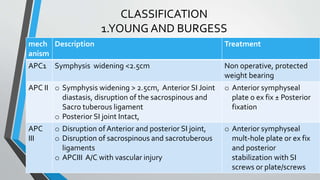
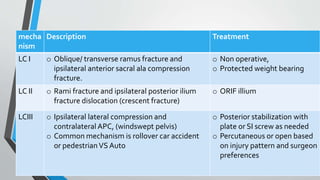
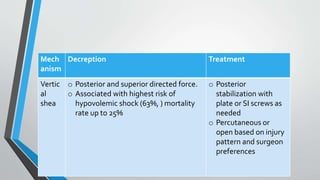
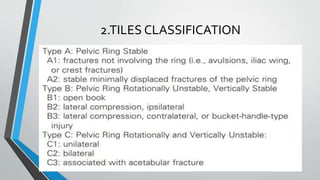
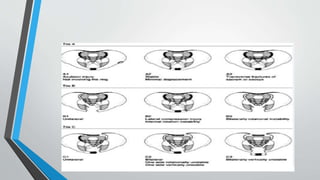
- Classification systems include Young-Burgess and Tile systems.
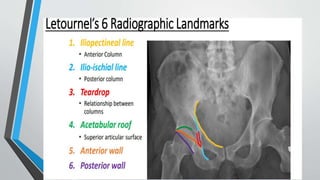
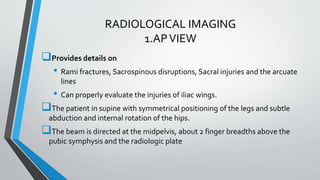
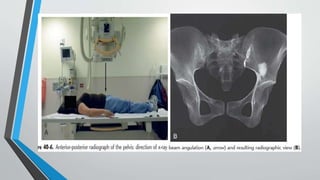
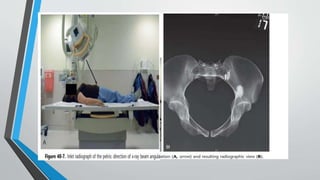
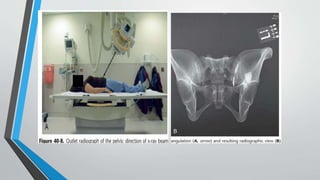
- Imaging includes x-rays, CT, MRI and scintigraphy to evaluate injuries.
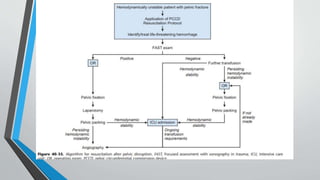
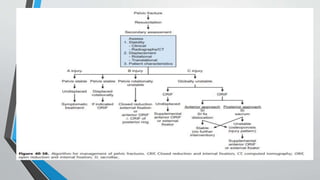
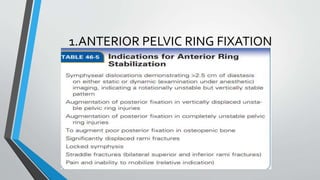
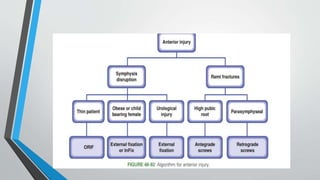
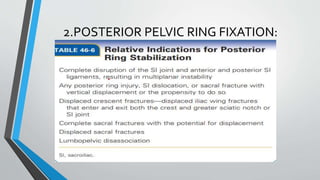
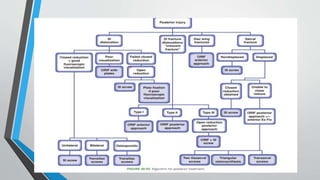
- Treatment involves stabilizing fractures through external or internal fixation depending on fracture pattern and hemodynamic stability of the patient.