This document discusses pediatric contact lens management and fitting considerations. Key points include:
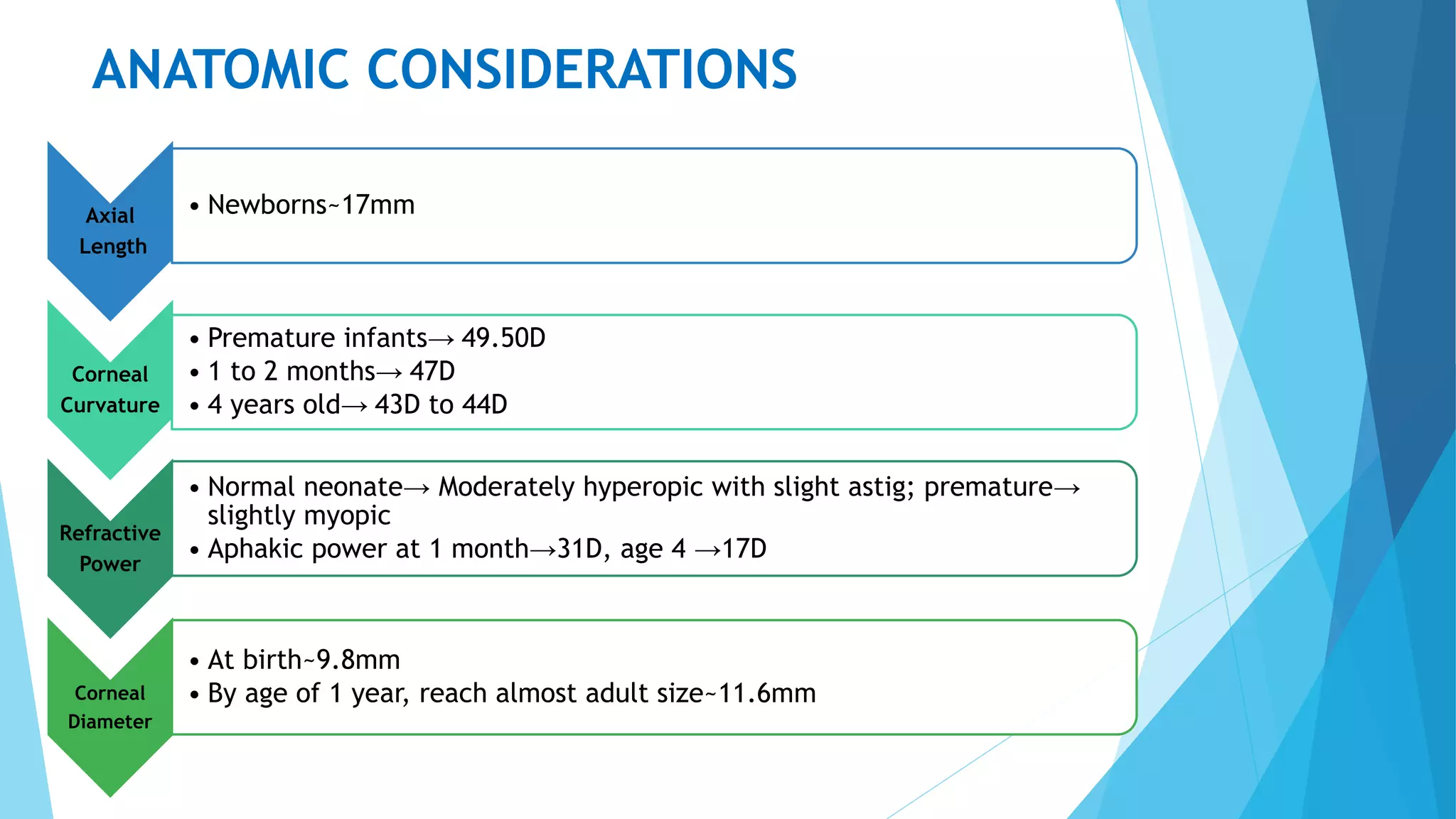
- Anatomical considerations for pediatric eyes such as shorter axial length and steeper corneal curvature compared to adults.
- Indications for pediatric contact lens fitting include high refractive errors, aphakia, and irregular astigmatism.
- Silicone elastomer, hydrogel, and RGP lenses are commonly used in pediatric fittings, each with advantages and disadvantages.
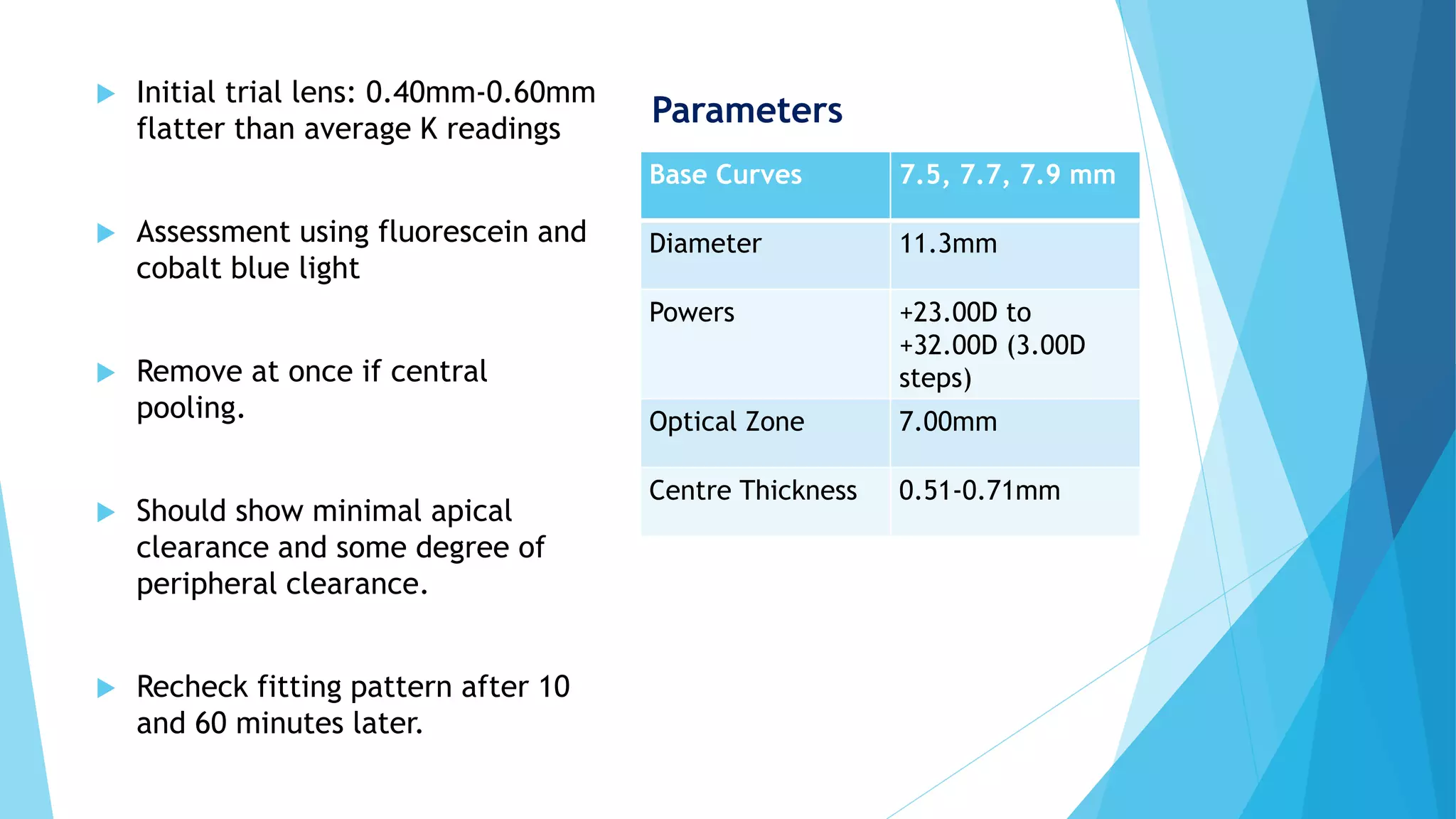
- A thorough prefitting exam evaluates lid and corneal health before determining initial lens parameters based on age.
- Fitting is assessed using fluorescein pattern and lens movement, with progress evaluated regularly according to age.






















![Types of pediatric contact lens [autosaved]](https://cdn.slidesharecdn.com/ss_thumbnails/typesofpediatriccontactlensautosaved-200210123904-thumbnail.jpg?width=640&height=640&fit=bounds)


















































![contact lenses in children[1].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/contactlensesinchildren1-230805101331-3467ad8b-thumbnail.jpg?width=640&height=640&fit=bounds)



























