HISTORY OF CONTACTLENS
1508, Leonardo Da Vinci used bowl half
filled with water.
1637, Descartes used tube filled with water.
1887, Muller used glass shell
1888, Fick formulated term C.L
Initially 2 types were available-
- Blown glass lens from Muller
- Ground glass lens from Zeiss
1937, Feinbloom 1st used plastic polymer for
manufacture
1938 – Orbig & Muller – Transparent MMA
1946 – PMMA CL
1948 – Plastic CL – Kevin Tuchy
1961 – Hydrophilic CL - HEMA CL - Wichterle
4.
CLASSIFICATION
ANATOMICAL POSITION
I.Scleral contact lens
II. Semi-scleral contact lens
III. Corneal contact lens
NATURE OF LENS MATERIAL
I. Rigid non-gas permeable/hard C.L.
(PMMA)
II. Rigid gas permeable/semi-soft C.L.
(Cellulose acetate butyrate - CAB)
III. Soft C.L. (HEMA).
5.
CLASSIFICATION
MODE OF WEAR
I. Daily wear
II. Extended wear
III. Disposable
PURPOSE OF USE
I. Optical
II. Therapeutic
III. Cosmetic
WATER CONTENT
• Low (0-40%)
• Medium (40-55%)
• High (>55%)
6.
DESIGN
1. Singlecut lens -
single continuous front surface
back surface – base curve and peripheral curve
2. Lenticular cut lens
Front surface- central optic portion surrounded by peripheral carrier
portion
WETTABILITY
Adherence ofliquid to surface of solid despite of cohesive forces holding liquid
together
The angle that the edge of a bead of water makes with the surface of a contact
lens called a wetting angle.
The smaller the wetting angle the greater the wettability of lens.
Complete wetting – wetting angle 0’
Partial wetting – wetting angle 70’
Non wetting – wetting angle 150’
9.
OXYGEN TRANSMISSIBILITY
DK/L
D=Diffusion coefficient (cm/sec)
K=solubility of gas in material(cm3/cm2mmhg)
L= thickness of material(mm)
Depends on:
permeability of lens material
Thickness of lens
Temperature at which test is performed
10.
OXYGEN PERMEABILITY
LowDk material
Below 20
Mid Dk material
20 to 40
High Dk material
40 to 60
Hyper Dk material
Above 60
Property of the polymeric material to
transmit gaseous substances
Unit from which O2 passage for a specific
lens is derived
11.
OXYGEN PERMEABILITY
Dailywear, the recommended Dk/L of a contact lens is around 30
Low oxygen transmissibility can result in corneal changes:
- Microcysts
- Polymegathism
- Corneal Ph
- Edema
- Blebs
12.
IDEAL MATERIAL
BIOCOMPATIBILITY
Should not harmful
OPTICAL PROPERTY
Transparency
Refractive index approximating to tears
Gas permeability
Tolerance
Moulding
Sterility
Stability
Surface chemistry – wettable – cover by tears
THERAPEUTIC
Trichiasis /entropion
Post pterygium operation
Dry eye syndrome
For drug delivery(glaucoma)
Melanosis of conjunctiva – use to deliver high dose continuous to conjunctiva
In glaucoma –vehicle for drug delivery
Amblyopia – opaque CL for occlusion
ADVANTAGES OVER SPECTACLES
No peripheral aberration
No chromatic aberration
Prism distortion can be controlled
Less minification / magnification
Astigmatism can controlled
No fogging
Increases field of vision
Cosmetically more pleasant
BSV in high anisometropia (u/l amblyopia)
HARD CONTACT LENS
(RIGIDNON-GAS PERMEABLE LENS)
Made of PMMA.
Confirm to the cornea.
ADVANTAGE
Light in weigh
High optical quality
Non toxic
Easy to manufacture
27.
HARD CONTACT LENS
(RIGIDNON-GAS PERMEABLE LENS)
DISADVANTAGE
Low wettability
Low O2 permeability (DK value = 0)
Hard
Now obsolete
28.
RIGID GAS PERMIABLELENS
(RGP) / SEMI SOFT LENS
Initially made of Cellulose Acetate Butyrate.
Silicon Acrylate
Copolymer of PMMA & Silicon containing vinyl monomer
Styrene
Fluropolymers-for extended wear.
Size- usually 9-10mm.
Best in high myopes, astigmatism >2d, keratoconus.
29.
SOFT CONTACT LENS
HIGHWATER CONTENT
Up to 85 % of H2O
Made of hydrogel
HEMA
HEMA-VP (Vinyl pyrrolidone)
LENSES –max hydration 45%
MMA-PVD LENSES
Glycidyl methacrylate
LOW WATER CONTENT
38 – 45 % of H2O
High DK value
Made of silicone hydrogel
30.
SOFT CONTACT LENS
HIGHWATER CONTENT
Advantage
Higher DK
More flexible
Faster restoration of shape following
deformation.
Disadvantage
More fragile
More deposit prone
Difficult to manufacture
Lower tensile strength
Cannot be made too thin
LOW WATER CONTENT
Advantage
Less susceptible to environment changes
Low protein deposition
Ease of manufacture
More wettable
Compatible with all lens care product
Disadvantage
Low DK
Less flexible
Thin lens difficult to handle
31.
ADVANTAGES OF RIGIDCONTACT LENS
Better quality of vision
More durable
Correction of astigmatism
Deposit resistance
Less of chance of infection
Cost of lens
Less comfortable, tough
32.
ADVANTAGE OF SOFTCONTACT LENS
Very comfortable and easy to adapt
Larger & adhere more tightly to the cornea
No spectacle blur
Doesn’t correct astigmatism
33.
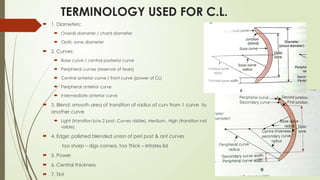
TERMINOLOGY USED FORC.L.
1. Diameters:
Overall diameter / chord diameter
Optic zone diameter
2. Curves:
Base curve / central posterior curve
Peripheral curves (reservoir of tears)
Central anterior curve / front curve (power of CL)
Peripheral anterior curve
Intermediate anterior curve
3. Blend: smooth area of transition of radius of curv from 1 curve to
another curve
Light (transition b/w 2 post. Curves visible), Medium , High (transition not
visible)
4. Edge: polished blended union of peri post & ant curves
too sharp – digs cornea, too Thick – irritates lid
5. Power
6. Central thickness
7. Tint
34.
CONTACT LENS FITTING
PRE-FITCONSULTATION
Complete history
Detailed eye examination
KERATOMETRIC METHOD
Pupil diameter [with IPD scale] is measured.
HVID is measured.
Corneal diameter is measured.
Radius of curvature is measured with a keratometer.
35.
CONTACT LENS FITTING
KERATOMETRICMETHOD
BASE CURVE, back surface of lens.
Rest on cornea responsible for good fit.
Long radius of curvature – flatter base curve.
TD depends upon lid diameter & corneal diameter OR HVID.
Optical zone should be at least 7 mm.
Posterior surface – Aspheric.
Anterior surface –convex with power.
36.
CONTACT LENS FITTING
TRIALLENS METHOD
Various lens from trial set tried until appropriate B.C. achieved.
Very tedious and cumbersome
A large trial set has to be maintained
INVENTORY FITTING METHOD
Combination of both above
More time efficient and more convenient to patient.
37.
FACTORS TO BEKEPT IN MIND
The total diameter should 1-1.5 mm greater than HVID.
BC should be 0.3-0.6 mm flatter than the flattest k reading.
DETERMINATION OF LENS POWER
• Spherical power + ½ cylindrical power [ if cyl is b/w 0.5D to 2.00D ]
• If cyl is < 0.5D Drop cylinder.
• If cyl is > 2.00D , go for toric CL.
38.
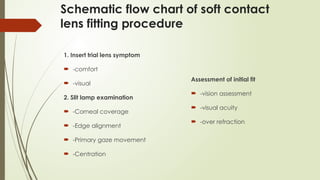
EVALUATION OF TRIALLENS FIT
1. Position of lens: (optic zone must cover pupillary area)
Lens Ride high- upper edge of lens crosses upper limbus in straight gaze
Higher position of lowerlid – reduce diameter of lens
Tight upper lid –Thin edge will slip under upper lid
Large lens / with the rule astigmatism – small or steep lens
Lens ride low – lower edge touches the limbus
Lens heavy (single cut aphakic lens)– making minus carrier lens
Lens small/flat – large or steep lens
Exophthalmos - large lens / steep& small lens
39.
EVALUATION OF TRIALLENS FIT
2. Base curve determination – Tear exchange - pumping action - Blinking
Flat base curve
Excess lens movement
High / low riding / horizontal
Flourescein pattern
Corneal abrasion, irregularity, distortion
Steep base curve
Little or no movement
Air-bubble under surface of lens
Flourescein pattern
Burning sensation, edema, hazy vision
Ideal base curve
40.
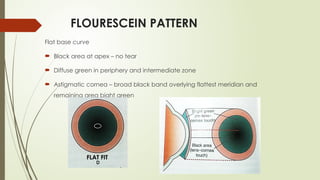
FLOURESCEIN PATTERN
Flat basecurve
Black area at apex – no tear
Diffuse green in periphery and intermediate zone
Astigmatic cornea – broad black band overlying flattest meridian and
remaining area bight green
FLAT FIT
41.
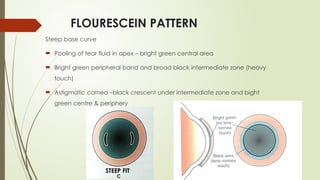
FLOURESCEIN PATTERN
Steep basecurve
Pooling of tear fluid in apex – bright green central area
Bright green peripheral band and broad black intermediate zone (heavy
touch)
Astigmatic cornea –black crescent under intermediate zone and bight
green centre & periphery
STEEP FIT
42.
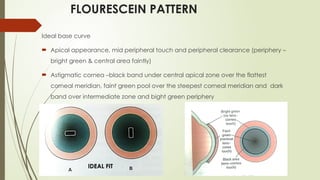
FLOURESCEIN PATTERN
Ideal basecurve
Apical appearance, mid peripheral touch and peripheral clearance (periphery –
bright green & central area faintly)
Astigmatic cornea –black band under central apical zone over the flattest
corneal meridian, faint green pool over the steepest corneal meridian and dark
band over intermediate zone and bight green periphery
IDEAL FIT
43.
EVALUATION OF TRIALLENS FIT
1. Base curve evaluation: (fluorescein is never used in soft CL)
a) Movement of lens over cornea: <0.5-1mm, flat/loose fit moves rapid, steep /tight fit
doesn’t move
b) Centring – proper fitting will centre well
c) Effect of blinking – Visual acuity, retinoscopic reflex, keratometermires
steep fit – clears after blink
flat fit – blurs after blink
d) Compression of blood vessels, indentation on sclera
2. Diameter evaluation: diameter should extend 1-1.5 mm over cornea
3. Lens power evaluation: clear vision
44.
LENS WITH IDEALBASE CURVE
1. Maintains 0.5-1.0 mm movement
2. Movements good centration
3. Doesnot cause compression of the conj. Vessels
4. Maintains stable VA with and without blinking
5. Maintains sharp and crisp retinoscopic reflex and keratometric mires before
and after blinking
RIGID LENS PROBLEMS
Blurred vision – Distance:
Blurred vision – Near:
Blurred vision – when wearing specs:
Awareness of presence of lens:
Burn, hot & scratchy eyes
Lens touching eyelids
Discomfort in morning
Tilting back of head
Excess blinking
Swelling of lid in evening
Difficulty in removing
Lens fall out frequently
Discomfort in eye movements
Photophobia
Watering
Pain
47.
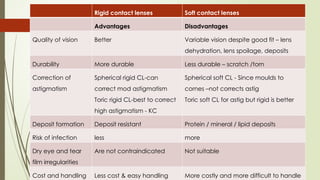
Rigid contact lensesSoft contact lenses
Advantages Disadvantages
Quality of vision Better Variable vision despite good fit – lens
dehydration, lens spoilage, deposits
Durability More durable Less durable – scratch /torn
Correction of
astigmatism
Spherical rigid CL-can
correct mod astigmatism
Toric rigid CL-best to correct
high astigmatism - KC
Spherical soft CL - Since moulds to
cornes –not corrects astig
Toric soft CL for astig but rigid is better
Deposit formation Deposit resistant Protein / mineral / lipid deposits
Risk of infection less more
Dry eye and tear
film irregularities
Are not contraindicated Not suitable
Cost and handling Less cost & easy handling More costly and more difficult to handle
48.
Rigid contact lensesSoft contact lenses
Disadvantages Advantages
Comfort Less comfortable and more
difficult to adapt
Very comfortable and more
easy to adapt
Wearing
problems
Prob with irregular schedule
Over wear - pain
Intermittent wear – no
problem
Over wear – less severe
Spectacle blur May occur Not occur
Lens stability Less eye stability, lost
frequently
Larger & adhere more tightly
and so dislodges less freq
49.
WEAR AND REPLACEMENTSCHEDULE
DW-daily wear:
• Traditional replacement cycle> 3 months
• Monthly replacement
• Daily replacement
EW-extended wear: Allowing lenses to be worn for 7 days/6 nights without
removal.
During one night per week the eyes are free of lenses. Weekly replaced by new
lenses
50.
WEAR AND REPLACEMENTSCHEDULE
FW-Flexible wear: Compromise between DW & EW.
Depending upon the demand of the patient to once a while sleep in lenses
51.
HYBRID RGPs
Centraloptical zone, formed by Rigid GP ,surrounded by peripheral soft
contact lens material.
Second generation silicone hydrogel CL, called Duette, having highly
oxygen permeable GP centre , surrounded by a soft silicone hydrogel “skirt”
for comfort.
52.
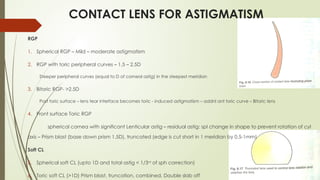
CONTACT LENS FORASTIGMATISM
RGP
1. Spherical RGP – Mild – moderate astigmatism
2. RGP with toric peripheral curves – 1.5 – 2.5D
Steeper peripheral curves (equal to D of corneal astig) in the steepest meridian
3. Bitoric RGP- >2.5D
Post toric surface – lens tear interface becomes toric - induced astigmatism – addnl ant toric curve – Bitoric lens
4. Front surface Toric RGP
spherical cornea with significant Lenticular astig – residual astig: spl change in shape to prevent rotation of cyl
axis – Prism blast (base down prism 1.5D), truncated (edge is cut short in 1 meridian by 0.5-1mm)
Soft CL
5. Spherical soft CL (upto 1D and total astig < 1/3rd
of sph correction)
6. Toric soft CL (>1D) Prism blast, truncation, combined, Double slab off
53.
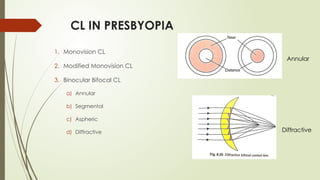
CL IN PRESBYOPIA
1.Monovision CL
2. Modified Monovision CL
3. Binocular Bifocal CL
a) Annular
b) Segmental
c) Aspheric
d) Diffractive
Annular
Diffractive
54.
ORTHOKERATOLOGY
Reversible andnoninvasive technique of reshaping cornea by wearing
specially designed RGP lenses over a period of time
Correction of Myopia
Overnight Ortho K lenses- worn during sleep 8hrs - Corneal flattening – need
not wear in day time
Effect is temporary and return to original shape if discontinued
FDA approved for myopia correction – corneal refractive lenses
55.
SPECIAL CONTACT LENS
COSMETICCONTACT LENS
1. TINTED LENS-
Can be opaque OR transparent
Used for cosmetic purpose
2. PAINTED LENS-
Painted with pigment to stimulate iris
Useful in occlusion therapy, disfigured cornea, vision-disturbing conditions such
as albinism, aniridia , iris coloboma.
56.
TYPES OF COSMETICLENSES
A. Iris painted with clear pupil [Albinotic lens]
B. Black pupil and iris painted
C. Pupil painted
DISADVANTAGE
Toxic effect
Corneal edema
57.
CONTACT LENS FORCOLOUR
BLINDNESS
Using customize filters to change the wavelength of each color.
Example- X-Chrome lens, Golden yellow lens
58.
FUTURE ADVANCES
AntibacterialCL – resist contamination
Soft CL – that slow progress of Myopia
Customised CL – correct individual ocular irregularities
CLs with embedded circuit - For monitoring IOP in glaucoma
CL measuring glucose levels in DM
Drug delivery CL
3D Cl for gaming
SIGN OF TIGHTFIT
Lens coverage-uniform
Movement <0.5 mm
Fluctuating vision clears on blinking
Progressive discomfort on wearing
Circumciliary congestion
Edge indentation of limbus
Retinoscopic image is fuzzy
To correct this-
Increase B.C. by 0.2-0.3 mm
Decrease T.D. by 0.5 mm
68.
SIGN OF LOOSEFIT
Poor centration
Movement >1 mm
Variable vision blurs on blinking
Edges stand off , ejection of lens
Retinoscopic image blur on blinking
To correct this-
Increase T.D. by 0.5-1 mm
Decrease B.C. by 0.2-0.3 mm


![THERAPEUTIC
[ BANDAGE SOFT C.L.]
Decreases pain
Prevent mechanical trauma by touch
Increases proper hydration and proper healing
Corneal edema
Corneal perforation
Corneal burns
Corneal grafts](https://image.slidesharecdn.com/contactlensdrhari-250828080058-f04461af/85/Contact-Lens-Dr-Hari-pptx-powerpoint-ppt-16-320.jpg)
![THERAPEUTIC
[ BANDAGE SOFT C.L.]
Bullous keratopathy
Leaking conjunctival blebs
Keratitis
Symblepharon
Lagophthalmos
Chronic and indolent ulcer](https://image.slidesharecdn.com/contactlensdrhari-250828080058-f04461af/85/Contact-Lens-Dr-Hari-pptx-powerpoint-ppt-17-320.jpg)


![CONTACT LENS FITTING
PRE-FIT CONSULTATION
Complete history
Detailed eye examination
KERATOMETRIC METHOD
Pupil diameter [with IPD scale] is measured.
HVID is measured.
Corneal diameter is measured.
Radius of curvature is measured with a keratometer.](https://image.slidesharecdn.com/contactlensdrhari-250828080058-f04461af/85/Contact-Lens-Dr-Hari-pptx-powerpoint-ppt-34-320.jpg)
![FACTORS TO BE KEPT IN MIND
The total diameter should 1-1.5 mm greater than HVID.
BC should be 0.3-0.6 mm flatter than the flattest k reading.
DETERMINATION OF LENS POWER
• Spherical power + ½ cylindrical power [ if cyl is b/w 0.5D to 2.00D ]
• If cyl is < 0.5D Drop cylinder.
• If cyl is > 2.00D , go for toric CL.](https://image.slidesharecdn.com/contactlensdrhari-250828080058-f04461af/85/Contact-Lens-Dr-Hari-pptx-powerpoint-ppt-37-320.jpg)



![TYPES OF COSMETIC LENSES
A. Iris painted with clear pupil [Albinotic lens]
B. Black pupil and iris painted
C. Pupil painted
DISADVANTAGE
Toxic effect
Corneal edema](https://image.slidesharecdn.com/contactlensdrhari-250828080058-f04461af/85/Contact-Lens-Dr-Hari-pptx-powerpoint-ppt-56-320.jpg)































![Optics of contact lens and nomenclature copy [repaired] (1)](https://cdn.slidesharecdn.com/ss_thumbnails/opticsofcontactlensandnomenclature-copyrepaired1-170218054900-thumbnail.jpg?width=640&height=640&fit=bounds)
































