
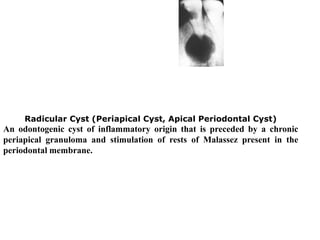

This document discusses various topics related to pediatric oral surgery including: 1. Extraction techniques for both primary and permanent teeth in children. It describes the appropriate forceps and methods for extracting different types of teeth. 2. Management of impacted and supernumerary teeth including indications for removal and surgical techniques. 3. Treatment of common odontogenic infections in children such as apical abscesses. 4. Pre-operative preparation and obtaining consent when performing procedures on children.























































































